
Page 110 - HIVMED_v21_i1.indb
P. 110
Page 19 of 34 Guideline
other people engaged in illegal and/or stigmatised practices services hold true particularly for people who use licit drugs
could be developed to quantify stigma and measure changes in countries where drug use has been criminalised and where
over time. no harm reduction services exist. To address the concerns
emerging from the many interacting aspects of violence,
Clinicians should ensure that the health services they provide trauma and substance use, harm-reducing systems of care
109
are available, accessible and acceptable to people who use need to integrate with other primary healthcare services.
drugs. Linking harm reduction services to services such as sexual
and reproductive health (SRH) services, including sexually
Approaches to rendering services friendly to people who use transmitted infection (STI) prevention services, and
drugs and other key populations: supportive primary care would allow for more effective
• Ensuring adequate training of staff and develop harm reduction programming.
supportive attitudes towards people who use drugs
• Integrating health services 3. Special considerations
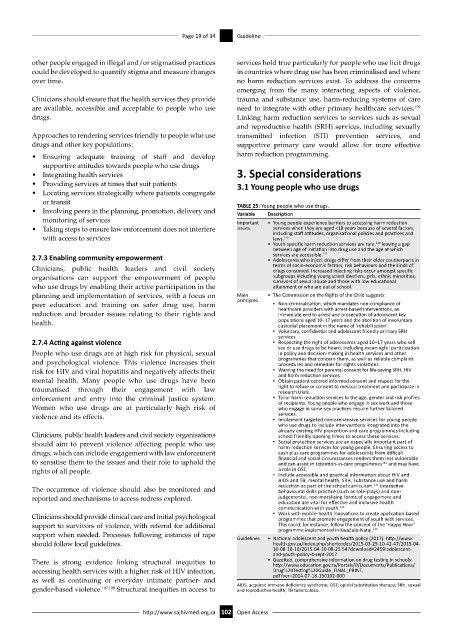
• Providing services at times that suit patients 3.1 Young people who use drugs
• Locating services strategically where patients congregate
or transit TABLE 25: Young people who use drugs.
• Involving peers in the planning, promotion, delivery and Variable Description
monitoring of services Important • Young people experience barriers to accessing harm reduction
• Taking steps to ensure law enforcement does not interfere issues services when they are aged <18 years because of several factors,
with access to services including staff attitudes, organisational policies and practices and
laws.
110
• Youth-specific harm reduction services are rare, leaving a gap
110
between age of initiation into drug use and the age at which
services are accessible.
111
2.7.3 Enabling community empowerment • Adolescents who inject drugs differ from their older counterparts in
Clinicians, public health leaders and civil society terms of socio-economic factors, risk behaviours and the kinds of
drugs consumed. Increased injecting risks occur amongst specific
organisations can support the empowerment of people subgroups including young street dwellers, girls, ethnic minorities,
survivors of sexual abuse and those with low educational
who use drugs by enabling their active participation in the attainment or who are out of school.
planning and implementation of services, with a focus on Main • The Commission on the Rights of the Child suggests:
peer education and training on safer drug use, harm principles ▪ Non-criminalisation, which mandates non-compliance of
healthcare providers with arrest-based interventions, an
reduction and broader issues relating to their rights and immediate end to arrest and prosecution of adolescent key
health. populations aged 10–17 years and the abolition of involuntary
custodial placement in the name of ‘rehabilitation’.
▪ Voluntary, confidential and adolescent friendly primary SRH
services
2.7.4 Acting against violence ▪ Respecting the right of adolescents aged 10–17 years who sell
sex or use drugs to be heard, including meaningful participation
People who use drugs are at high risk for physical, sexual in policy and decision-making in health services and other
and psychological violence. This violence increases their programmes that concern them, as well as reliable complaint
procedures and remedies for rights violations.
risk for HIV and viral hepatitis and negatively affects their ▪ Waiving the need for parental consent for life-saving SRH, HIV
and harm reduction services.
mental health. Many people who use drugs have been ▪ Obtain patient-centred informed consent and respect for the
traumatised through their engagement with law right to refuse or consent to medical treatment and participate in
research trials.
enforcement and entry into the criminal justice system. ▪ Tailor harm reduction services to the age, gender and risk profiles
of recipients. Young people who engage in sex work and those
Women who use drugs are at particularly high risk of who engage in same-sex practices require further tailored
services.
violence and its effects. ▪ Implement targeted comprehensive services for young people
who use drugs to include interventions integrated into the
already existing HIV prevention and care programmes including
Clinicians, public health leaders and civil society organisations school friendly opening times to access these services.
should aim to prevent violence affecting people who use ▪ Social protection services are an especially important part of
harm reduction services for young people. Ensuring access to
drugs, which can include engagement with law enforcement cash plus care programmes for adolescents from difficult
to sensitise them to the issues and their role to uphold the financial and social circumstances renders them less vulnerable
and can assist in retention-in-care programmes and may have
112
rights of all people. a role in OST.
▪ Include accessible and practical information about HIV and
AIDS and TB, mental health, SRH, substance use and harm
111
The occurrence of violence should also be monitored and reduction as part of the school curriculum. Interactive
behavioural skills practice (such as role-plays) and non-
reported and mechanisms to access redress explored. judgemental, non-moralising forms of engagement and
education are vital for effective and inclusive health
communication with youth. 111
Clinicians should provide clinical care and initial psychological ▪ Work with mobile-health innovations to create application-based
programmes that promote engagement of youth with services.
support to survivors of violence, with referral for additional This could, for instance, follow the concept of the ‘Happy Hour’
programme implemented in KwaZulu-Natal.
112
support when needed. Processes following instances of rape Guidelines • National adolescent and youth health policy (2017): http://www.
should follow local guidelines. health.gov.za/index.php/shortcodes/2015-03-29-10-42-47/2015-04-
30-08-18-10/2015-04-30-08-25-54?download=2459:adolescent-
and-youth-policy-4-sept-2017
There is strong evidence linking structural inequities to • Gazetted, comprehensive information on drug testing in schools:
http://www.education.gov.za/Portals/0/Documents/Publications/
accessing health services with a higher risk of HIV infection, Drug%20Testing%20Guide_FINAL_PRINT.
as well as continuing or everyday intimate partner- and pdf?ver=2014-07-18-150102-000
gender-based violence. 107,108 Structural inequities in access to AIDS, acquired immune deficiency syndrome; OST; opioid substitution therapy; SRH, sexual
and reproductive health; TB tuberculosis.
http://www.sajhivmed.org.za 102 Open Access