
Page 47 - HIVMED_v21_i1.indb
P. 47
Page 21 of 39 Guideline
Viral load > 50 copies/mL
VL > 50 copies/mL and on
In patients on a second-line regimen containing a boosted Pl- or DTG-based second-line
PI, if the VL is not suppressed, then we do not advise ART regimen for >2 years
switching to DTG. We advise for enhanced adherence Adherence, tolerability drug
counselling and switching to an alternative boosted PI if interac ons, psychological issues
there is intolerance. If the VL subsequently re-suppresses to
an undetectable VL < 50 copies/mL, then the advice in the Repeat VL a er 2–3 months
section above should be followed. If the VL remains
elevated, then the patient may be eligible for a resistance
test, with consideration for a third-line therapy if they fulfil VL ≤ 500 copies/mL VL > 500 copies/mL
the criteria outlined in section 14.
14. Third-line antiretroviral therapy Continue second-line
ART regimen
Key points If VL is 50–500 copies/mL, Perform
then repeat in 3 months resistance
tes ng
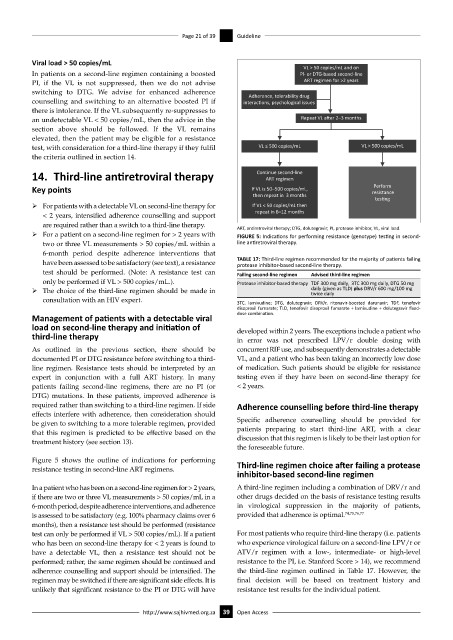
ÿ For patients with a detectable VL on second-line therapy for If VL < 50 copies/mL then
repeat in 6–12 months
< 2 years, intensified adherence counselling and support
are required rather than a switch to a third-line therapy. ART, antiretroviral therapy; DTG, dolutegravir; PI, protease inhibitor, VL, viral load.
ÿ For a patient on a second-line regimen for > 2 years with FIGURE 5: Indications for performing resistance (genotype) testing in second-
two or three VL measurements > 50 copies/mL within a line antiretroviral therapy.
6-month period despite adherence interventions that
have been assessed to be satisfactory (see text), a resistance TABLE 17: Third-line regimen recommended for the majority of patients failing
protease inhibitor-based second-line therapy.
test should be performed. (Note: A resistance test can Failing second-line regimen Advised third-line regimen
only be performed if VL > 500 copies/mL.). Protease inhibitor-based therapy TDF 300 mg daily, 3TC 300 mg daily, DTG 50 mg
ÿ The choice of the third-line regimen should be made in daily (given as TLD) plus DRV/r 600 mg/100 mg
twice daily
consultation with an HIV expert. 3TC, lamivudine; DTG, dolutegravir; DRV/r, ritonavir-boosted darunavir; TDF, tenofovir
disoproxil fumarate; TLD, tenofovir disoproxil fumarate + lamivudine + dolutegravir fixed-
Management of patients with a detectable viral dose combination.
load on second-line therapy and initiation of developed within 2 years. The exceptions include a patient who
third-line therapy in error was not prescribed LPV/r double dosing with
As outlined in the previous section, there should be concurrent RIF use, and subsequently demonstrates a detectable
documented PI or DTG resistance before switching to a third- VL, and a patient who has been taking an incorrectly low dose
line regimen. Resistance tests should be interpreted by an of medication. Such patients should be eligible for resistance
expert in conjunction with a full ART history. In many testing even if they have been on second-line therapy for
patients failing second-line regimens, there are no PI (or < 2 years.
DTG) mutations. In these patients, improved adherence is
required rather than switching to a third-line regimen. If side Adherence counselling before third-line therapy
effects interfere with adherence, then consideration should
be given to switching to a more tolerable regimen, provided Specific adherence counselling should be provided for
that this regimen is predicted to be effective based on the patients preparing to start third-line ART, with a clear
treatment history (see section 13). discussion that this regimen is likely to be their last option for
the foreseeable future.
Figure 5 shows the outline of indications for performing Third-line regimen choice after failing a protease
resistance testing in second-line ART regimens.
inhibitor-based second-line regimen
In a patient who has been on a second-line regimen for > 2 years, A third-line regimen including a combination of DRV/r and
if there are two or three VL measurements > 50 copies/mL in a other drugs decided on the basis of resistance testing results
6-month period, despite adherence interventions, and adherence in virological suppression in the majority of patients,
is assessed to be satisfactory (e.g. 100% pharmacy claims over 6 provided that adherence is optimal. 74,75,76,77
months), then a resistance test should be performed (resistance
test can only be performed if VL > 500 copies/mL). If a patient For most patients who require third-line therapy (i.e. patients
who has been on second-line therapy for < 2 years is found to who experience virological failure on a second-line LPV/r or
have a detectable VL, then a resistance test should not be ATV/r regimen with a low-, intermediate- or high-level
performed; rather, the same regimen should be continued and resistance to the PI, i.e. Stanford Score > 14), we recommend
adherence counselling and support should be intensified. The the third-line regimen outlined in Table 17. However, the
regimen may be switched if there are significant side effects. It is final decision will be based on treatment history and
unlikely that significant resistance to the PI or DTG will have resistance test results for the individual patient.
http://www.sajhivmed.org.za 39 Open Access