
Page 45 - HIVMED_v21_i1.indb
P. 45
Page 19 of 39 Guideline
TABLE 14: Recommended second-line regimen in patients who have failed a
Pa ent on first-line regimen of two nucleoside reverse transcriptase inhibitors + non-
two NRTls + DTG nucleoside reverse transcriptase inhibitor.
Failing first-line regimen Advised second-line regimen
TDF + 3TC (or FTC) + NNRTI AZT + 3TC + DTG‡
VL every 6 months AZT + 3TC + NNRTI Resistance test: if fully active NRTI is available, then
(can be reduced to 12-monthly if suppresed) combine this with:
3TC (or FTC) + DTG, or TDF + FTC + DRV/r†
ABC + 3TC + NNRTI AZT + 3TC + DTG‡
NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase
• Enhanced adherence inhibitor; TDF, tenofovir disoproxil fumarate; 3TC, lamivudine; AZT, zidovudine; ABC,
VL < 50 VL > 50 counselling abacavir; DTG, dolutegravir; FTC, emtricitabine; DRV, darunavir.
copies/mL copies/mL • Address poten al side effects †, Provided that the patient has not potentially previously experienced virological failure on
affec ng adherence TDF, and has not experienced TDF nephrotoxicity previously.
‡, If the patient has chronic hepatitis B, then continue TDF, in addition, in the second-line
regimen.
Repeat VL
in 3 months second-line therapy. In this trial, a second-line regimen of
17
DTG + two NRTIs was superior in terms of virological
Con nue If VL > 500 copies/mL, then consider resistance suppression and better tolerated than LPV/r + two NRTIs
regimen in patients who had failed a first-line regimen of NNRTI +
testing in the case of:
• DTG monotherapy two NRTIs. An important caveat is that all patients enrolled
• Exposed to interacting drugs/drugs impairing
absorption without necessary adjustment in this trial had a resistance test performed at entry and had
• VL > 500 copies/mL for > 2 years despite 100% to have at least one fully active NRTI to be eligible for
adherence assessment
inclusion. Thus, the current evidence supports a DTG-based
Do not switch to second-line regimen unless regimen in second line only when used with at least one fully
resistance shown on resistance test
active NRTI. Whether a DTG-based second-line regimen
would be equally effective with two NRTIs when there is
DTG, dolutegravir; NRTIs, nucleoside reverse transcriptase inhibitors; VL; viral load. resistance to both those NRTIs is currently a knowledge gap
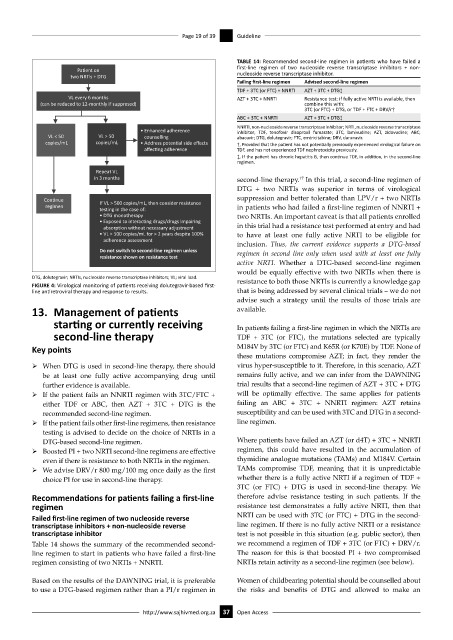
FIGURE 4: Virological monitoring of patients receiving dolutegravir-based first-
line antiretroviral therapy and response to results. that is being addressed by several clinical trials – we do not
advise such a strategy until the results of those trials are
13. Management of patients available.
starting or currently receiving In patients failing a first-line regimen in which the NRTIs are
second-line therapy TDF + 3TC (or FTC), the mutations selected are typically
Key points M184V by 3TC (or FTC) and K65R (or K70E) by TDF. None of
these mutations compromise AZT; in fact, they render the
ÿ When DTG is used in second-line therapy, there should virus hyper-susceptible to it. Therefore, in this scenario, AZT
be at least one fully active accompanying drug until remains fully active, and we can infer from the DAWNING
further evidence is available. trial results that a second-line regimen of AZT + 3TC + DTG
ÿ If the patient fails an NNRTI regimen with 3TC/FTC + will be optimally effective. The same applies for patients
either TDF or ABC, then AZT + 3TC + DTG is the failing an ABC + 3TC + NNRTI regimen: AZT retains
recommended second-line regimen. susceptibility and can be used with 3TC and DTG in a second-
ÿ If the patient fails other first-line regimens, then resistance line regimen.
testing is advised to decide on the choice of NRTIs in a
DTG-based second-line regimen. Where patients have failed an AZT (or d4T) + 3TC + NNRTI
ÿ Boosted PI + two NRTI second-line regimens are effective regimen, this could have resulted in the accumulation of
even if there is resistance to both NRTIs in the regimen. thymidine analogue mutations (TAMs) and M184V. Certain
ÿ We advise DRV/r 800 mg/100 mg once daily as the first TAMs compromise TDF, meaning that it is unpredictable
choice PI for use in second-line therapy. whether there is a fully active NRTI if a regimen of TDF +
3TC (or FTC) + DTG is used in second-line therapy. We
Recommendations for patients failing a first-line therefore advise resistance testing in such patients. If the
regimen resistance test demonstrates a fully active NRTI, then that
Failed first-line regimen of two nucleoside reverse NRTI can be used with 3TC (or FTC) + DTG in the second-
transcriptase inhibitors + non-nucleoside reverse line regimen. If there is no fully active NRTI or a resistance
transcriptase inhibitor test is not possible in this situation (e.g. public sector), then
Table 14 shows the summary of the recommended second- we recommend a regimen of TDF + 3TC (or FTC) + DRV/r.
line regimen to start in patients who have failed a first-line The reason for this is that boosted PI + two compromised
regimen consisting of two NRTIs + NNRTI. NRTIs retain activity as a second-line regimen (see below).
Based on the results of the DAWNING trial, it is preferable Women of childbearing potential should be counselled about
to use a DTG-based regimen rather than a PI/r regimen in the risks and benefits of DTG and allowed to make an
http://www.sajhivmed.org.za 37 Open Access