
Page 44 - HIVMED_v21_i1.indb
P. 44
Page 18 of 39 Guideline
clinical trials of DTG in first-line therapy, no DTG resistance
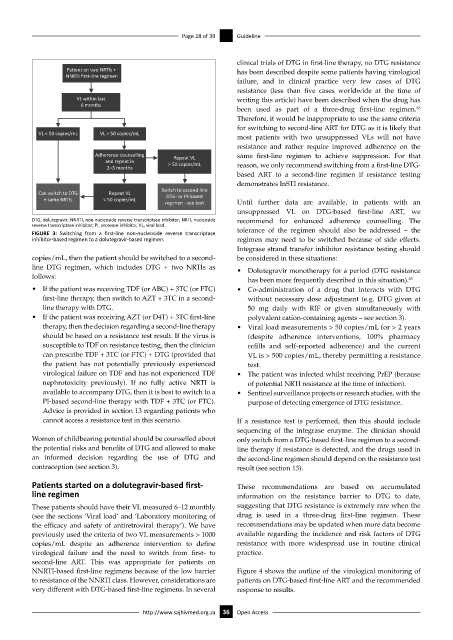
Pa ent on two NRTls + has been described despite some patients having virological
NNRTI first-line regimen
failure, and in clinical practice very few cases of DTG
resistance (less than five cases worldwide at the time of
VL within last writing this article) have been described when the drug has
6 months
been used as part of a three-drug first-line regimen.
63
Therefore, it would be inappropriate to use the same criteria
for switching to second-line ART for DTG as it is likely that
VL < 50 copies/mL VL > 50 copies/mL
most patients with two unsuppressed VLs will not have
resistance and rather require improved adherence on the
Adherence counselling Repeat VL same first-line regimen to achieve suppression. For that
and repeat in > 50 copies/mL reason, we only recommend switching from a first-line DTG-
2–3 months
based ART to a second-line regimen if resistance testing
demonstrates InSTI resistance.
Switch to second-line
Can switch to DTG Repeat VL DTG- or Pl-based
+ same NRTls < 50 copies/mL
regimen - see text Until further data are available, in patients with an
unsuppressed VL on DTG-based first-line ART, we
DTG, dolutegravir; NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside recommend for enhanced adherence counselling. The
reverse transcriptase inhibitor; PI, protease inhibitor, VL, viral load.
FIGURE 3: Switching from a first-line non-nucleoside reverse transcriptase tolerance of the regimen should also be addressed – the
inhibitor-based regimen to a dolutegravir-based regimen. regimen may need to be switched because of side effects.
Integrase strand transfer inhibitor resistance testing should
copies/mL, then the patient should be switched to a second- be considered in these situations:
line DTG regimen, which includes DTG + two NRTIs as • Dolutegravir monotherapy for a period (DTG resistance
follows:
has been more frequently described in this situation). 63
• If the patient was receiving TDF (or ABC) + 3TC (or FTC) • Co-administration of a drug that interacts with DTG
first-line therapy, then switch to AZT + 3TC in a second- without necessary dose adjustment (e.g. DTG given at
line therapy with DTG. 50 mg daily with RIF or given simultaneously with
• If the patient was receiving AZT (or D4T) + 3TC first-line polyvalent cation-containing agents – see section 3).
therapy, then the decision regarding a second-line therapy • Viral load measurements > 50 copies/mL for > 2 years
should be based on a resistance test result. If the virus is (despite adherence interventions, 100% pharmacy
susceptible to TDF on resistance testing, then the clinician refills and self-reported adherence) and the current
can prescribe TDF + 3TC (or FTC) + DTG (provided that VL is > 500 copies/mL, thereby permitting a resistance
the patient has not potentially previously experienced test.
virological failure on TDF and has not experienced TDF • The patient was infected whilst receiving PrEP (because
nephrotoxicity previously). If no fully active NRTI is of potential NRTI resistance at the time of infection).
available to accompany DTG, then it is best to switch to a • Sentinel surveillance projects or research studies, with the
PI-based second-line therapy with TDF + 3TC (or FTC). purpose of detecting emergence of DTG resistance.
Advice is provided in section 13 regarding patients who
cannot access a resistance test in this scenario. If a resistance test is performed, then this should include
sequencing of the integrase enzyme. The clinician should
Women of childbearing potential should be counselled about only switch from a DTG-based first-line regimen to a second-
the potential risks and benefits of DTG and allowed to make line therapy if resistance is detected, and the drugs used in
an informed decision regarding the use of DTG and the second-line regimen should depend on the resistance test
contraception (see section 3). result (see section 13).
Patients started on a dolutegravir-based first- These recommendations are based on accumulated
line regimen information on the resistance barrier to DTG to date,
These patients should have their VL measured 6–12 monthly suggesting that DTG resistance is extremely rare when the
(see the sections ‘Viral load’ and ‘Laboratory monitoring of drug is used in a three-drug first-line regimen. These
the efficacy and safety of antiretroviral therapy’). We have recommendations may be updated when more data become
previously used the criteria of two VL measurements > 1000 available regarding the incidence and risk factors of DTG
copies/mL despite an adherence intervention to define resistance with more widespread use in routine clinical
virological failure and the need to switch from first- to practice.
second-line ART. This was appropriate for patients on
NNRTI-based first-line regimens because of the low barrier Figure 4 shows the outline of the virological monitoring of
to resistance of the NNRTI class. However, considerations are patients on DTG-based first-line ART and the recommended
very different with DTG-based first-line regimens. In several response to results.
http://www.sajhivmed.org.za 36 Open Access