
Page 51 - HIVMED_v21_i1.indb
P. 51
Page 25 of 39 Guideline
BOX 4: Contacts and resources for seeking reliable information on drug–drug TABLE 19: Antiretroviral drug interactions with rifampicin and recommendations
interactions. for co-administration.
• Package inserts of ARVs and concomitant drugs Class ART drug Interaction Dose of ART drug with RIF
• University of Liverpool HIV Drug Interactions Checker: https://www.hiv-
druginteractions.org/checker NRTI All in class No significant pharmacokinetic No dose adjustment
• Aid for AIDS Clinical Guidelines contain tables giving advice on drug–drug interactions required
interactions: http://www.aidforaids.co.za/dp_clin.php NNRTI EFV Mild reduction in EFV No dose adjustment
• University of Cape Town (UCT) Medicines Information Centre (MIC) has a regularly concentrations required (600 mg nocte)
updated table of interactions between ARVs and drugs used in the public sector INH increases EFV
(essential medicines list): http://www.mic.uct.ac.za/sites/default/files/image_ concentrations in genetic slow
tool/images/51/EML-ART%20Interaction%20Booklet%20Feb%202019_0.pdf metabolisers (~20% of South
• UCT MIC HIV & TB Hotline: 0800 212 506 or 021 406 6782 Africans), who already have
high EFV concentrations – this
ARV, antiretroviral; HIV, human immunodeficiency virus; AIDS, acquired immune deficiency can result in toxicity
syndrome.
ETR and RPV Marked reduction in Do not prescribe
concentrations concomitantly with RIF
and when drugs are co-administered, using one or more of PI/r LPV/r LPV plasma concentrations Double the dose of LPV/r
the resources listed in Box 4. significantly decreased to 800 mg/200 mg
12 hourly
There is an increased risk
° Common pitfalls: of hepatotoxicity with this
adjustment can be made
° Not checking for interactions between concomitant strategy. The dose
drugs and current or newly initiated ARVs. gradually over 1–2 weeks.
Dose adjustment should be
Concomitant drugs may need dose adjustment or continued for 2 weeks after
RIF is stopped
discontinuation when ART is switched, for example, All other PI/r Significant reduction in PI Do not prescribe
switching from a moderate inducer (EFV) to a strong concentrations concomitantly
inhibitor (PI/r), or from either of these to an InSTI. InSTI RAL Reduction in concentrations Increase dose to 800 mg
12 hourly
° Not considering marked increases in statin
DTG Significant reduction in Increase dose frequency to
considerations when used concomitantly with PIs. concentrations 50 mg 12 hourly
There are major interactions between PIs and many CCR5 MVC Reduction in concentrations Increase MVC dose to
statins, which result in marked increases in statin blocker 600 mg twice daily when
co-administered with RIF in
concentrations. Low-dose atorvastatin (not exceeding the absence of a potent
CYP3A4 inhibitor
10 mg, which will give an equivalent exposure to ART, antiretroviral therapy; DTG, dolutegravir; EFV, efavirenz; ETR, etravirine; InSTI, integrase
about 60 mg) can be used with PIs, but simvastatin inhibitor (integrase strand transfer inhibitor); LPV, lopinavir; LPV/r, ritonavir-boosted
lopinavir; MVC, maraviroc; NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI,
cannot be used. nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; PI/r, ritonavir-boosted
protease inhibitors; RAL, raltegravir; RIF, rifampicin; RPV, rilpivirine; INH, isoniazid.
18. Tuberculosis These issues, which have recently been reviewed, affect
80
Key points decisions regarding the timing of ART in ART-naive patients
with TB (section 6).
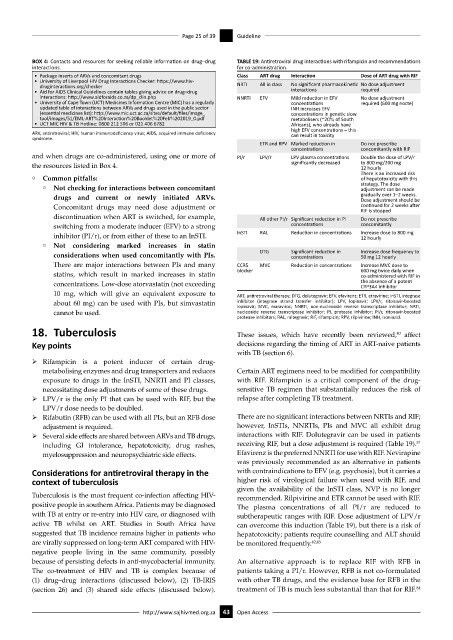
ÿ Rifampicin is a potent inducer of certain drug-
metabolising enzymes and drug transporters and reduces Certain ART regimens need to be modified for compatibility
exposure to drugs in the InSTI, NNRTI and PI classes, with RIF. Rifampicin is a critical component of the drug-
necessitating dose adjustments of some of these drugs. sensitive TB regimen that substantially reduces the risk of
ÿ LPV/r is the only PI that can be used with RIF, but the relapse after completing TB treatment.
LPV/r dose needs to be doubled.
ÿ Rifabutin (RFB) can be used with all PIs, but an RFB dose There are no significant interactions between NRTIs and RIF;
adjustment is required. however, InSTIs, NNRTIs, PIs and MVC all exhibit drug
ÿ Several side effects are shared between ARVs and TB drugs, interactions with RIF. Dolutegravir can be used in patients
81
including GI intolerance, hepatotoxicity, drug rashes, receiving RIF, but a dose adjustment is required (Table 19).
myelosuppression and neuropsychiatric side effects. Efavirenz is the preferred NNRTI for use with RIF. Nevirapine
was previously recommended as an alternative in patients
Considerations for antiretroviral therapy in the with contraindications to EFV (e.g. psychosis), but it carries a
context of tuberculosis higher risk of virological failure when used with RIF, and
given the availability of the InSTI class, NVP is no longer
Tuberculosis is the most frequent co-infection affecting HIV- recommended. Rilpivirine and ETR cannot be used with RIF.
positive people in southern Africa. Patients may be diagnosed The plasma concentrations of all PI/r are reduced to
with TB at entry or re-entry into HIV care, or diagnosed with subtherapeutic ranges with RIF. Dose adjustment of LPV/r
active TB whilst on ART. Studies in South Africa have can overcome this induction (Table 19), but there is a risk of
suggested that TB incidence remains higher in patients who hepatotoxicity; patients require counselling and ALT should
are virally suppressed on long-term ART compared with HIV- be monitored frequently. 82,83
negative people living in the same community, possibly
because of persisting defects in anti-mycobacterial immunity. An alternative approach is to replace RIF with RFB in
The co-treatment of HIV and TB is complex because of patients taking a PI/r. However, RFB is not co-formulated
(1) drug–drug interactions (discussed below), (2) TB-IRIS with other TB drugs, and the evidence base for RFB in the
84
(section 26) and (3) shared side effects (discussed below). treatment of TB is much less substantial than that for RIF.
http://www.sajhivmed.org.za 43 Open Access