
Page 37 - HIVMED_v21_i1.indb
P. 37
Page 11 of 39 Guideline
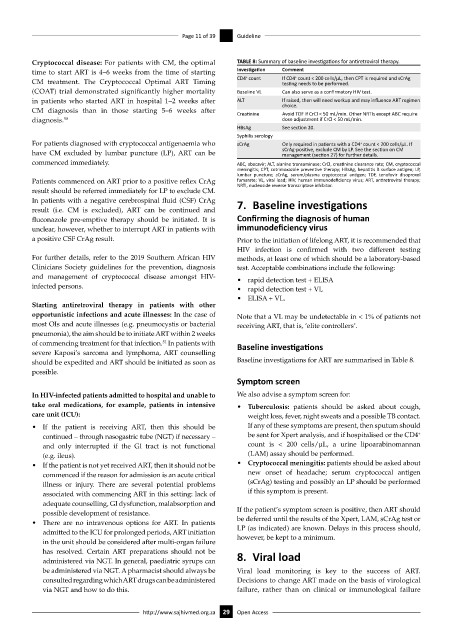
Cryptococcal disease: For patients with CM, the optimal TABLE 8: Summary of baseline investigations for antiretroviral therapy.
time to start ART is 4–6 weeks from the time of starting Investigation Comment
+
+
CM treatment. The Cryptococcal Optimal ART Timing CD4 count If CD4 count < 200 cells/μL, then CPT is required and sCrAg
testing needs to be performed.
(COAT) trial demonstrated significantly higher mortality Baseline VL Can also serve as a confirmatory HIV test.
in patients who started ART in hospital 1–2 weeks after ALT If raised, then will need workup and may influence ART regimen
CM diagnosis than in those starting 5–6 weeks after Creatinine choice.
Avoid TDF if CrCl < 50 mL/min. Other NRTIs except ABC require
diagnosis. 50 dose adjustment if CrCl < 50 mL/min.
HBsAg See section 20.
Syphilis serology
For patients diagnosed with cryptococcal antigenaemia who sCrAg Only required in patients with a CD4 count < 200 cells/μL. If
+
have CM excluded by lumbar puncture (LP), ART can be sCrAg-positive, exclude CM by LP. See the section on CM
management (section 27) for further details.
commenced immediately. ABC, abacavir; ALT, alanine transaminase; CrCl, creatinine clearance rate; CM, cryptococcal
meningitis; CPT, cotrimoxazole preventive therapy; HBsAg, hepatitis B surface antigen; LP,
lumbar puncture; sCrAg, serum/plasma cryptococcal antigen; TDF, tenofovir disoproxol
Patients commenced on ART prior to a positive reflex CrAg fumarate; VL, viral load; HIV, human immunodeficiency virus; ART, antiretroviral therapy;
NRTI, nucleoside reverse transcriptase inhibitor.
result should be referred immediately for LP to exclude CM.
In patients with a negative cerebrospinal fluid (CSF) CrAg 7. Baseline investigations
result (i.e. CM is excluded), ART can be continued and
fluconazole pre-emptive therapy should be initiated. It is Confirming the diagnosis of human
unclear, however, whether to interrupt ART in patients with immunodeficiency virus
a positive CSF CrAg result. Prior to the initiation of lifelong ART, it is recommended that
HIV infection is confirmed with two different testing
For further details, refer to the 2019 Southern African HIV methods, at least one of which should be a laboratory-based
Clinicians Society guidelines for the prevention, diagnosis test. Acceptable combinations include the following:
and management of cryptococcal disease amongst HIV- • rapid detection test + ELISA
infected persons. • rapid detection test + VL
• ELISA + VL.
Starting antiretroviral therapy in patients with other
opportunistic infections and acute illnesses: In the case of Note that a VL may be undetectable in < 1% of patients not
most OIs and acute illnesses (e.g. pneumocystis or bacterial receiving ART, that is, ‘elite controllers’.
pneumonia), the aim should be to initiate ART within 2 weeks
of commencing treatment for that infection. In patients with Baseline investigations
51
severe Kaposi’s sarcoma and lymphoma, ART counselling
should be expedited and ART should be initiated as soon as Baseline investigations for ART are summarised in Table 8.
possible.
Symptom screen
In HIV-infected patients admitted to hospital and unable to We also advise a symptom screen for:
take oral medications, for example, patients in intensive • Tuberculosis: patients should be asked about cough,
care unit (ICU): weight loss, fever, night sweats and a possible TB contact.
• If the patient is receiving ART, then this should be If any of these symptoms are present, then sputum should
+
continued – through nasogastric tube (NGT) if necessary – be sent for Xpert analysis, and if hospitalised or the CD4
and only interrupted if the GI tract is not functional count is < 200 cells/μL, a urine lipoarabinomannan
(e.g. ileus). (LAM) assay should be performed.
• If the patient is not yet received ART, then it should not be • Cryptococcal meningitis: patients should be asked about
commenced if the reason for admission is an acute critical new onset of headache; serum cryptococcal antigen
illness or injury. There are several potential problems (sCrAg) testing and possibly an LP should be performed
associated with commencing ART in this setting: lack of if this symptom is present.
adequate counselling, GI dysfunction, malabsorption and
possible development of resistance. If the patient’s symptom screen is positive, then ART should
• There are no intravenous options for ART. In patients be deferred until the results of the Xpert, LAM, sCrAg test or
admitted to the ICU for prolonged periods, ART initiation LP (as indicated) are known. Delays in this process should,
in the unit should be considered after multi-organ failure however, be kept to a minimum.
has resolved. Certain ART preparations should not be 8. Viral load
administered via NGT. In general, paediatric syrups can
be administered via NGT. A pharmacist should always be Viral load monitoring is key to the success of ART.
consulted regarding which ART drugs can be administered Decisions to change ART made on the basis of virological
via NGT and how to do this. failure, rather than on clinical or immunological failure
http://www.sajhivmed.org.za 29 Open Access