
Page 34 - HIVMED_v21_i1.indb
P. 34
Page 8 of 39 Guideline
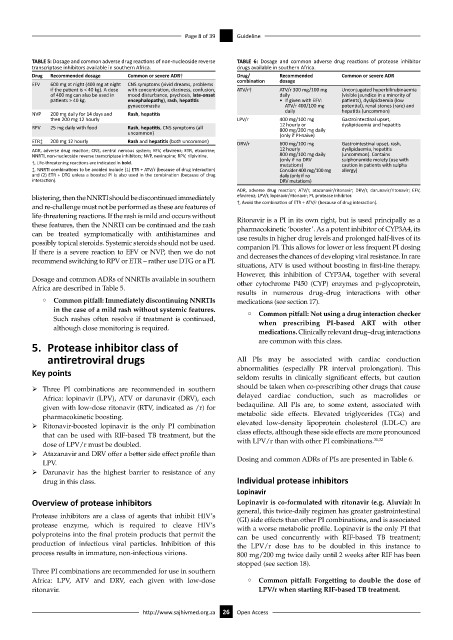
TABLE 5: Dosage and common adverse drug reactions of non-nucleoside reverse TABLE 6: Dosage and common adverse drug reactions of protease inhibitor
transcriptase inhibitors available in southern Africa. drugs available in southern Africa.
Drug Recommended dosage Common or severe ADR† Drug/ Recommended Common or severe ADR
EFV 600 mg at night (400 mg at night CNS symptoms (vivid dreams, problems combination dosage
if the patient is < 40 kg). A dose with concentration, dizziness, confusion, ATV/r† ATV/r 300 mg/100 mg Unconjugated hyperbilirubinaemia
of 400 mg can also be used in mood disturbance, psychosis, late-onset daily (visible jaundice in a minority of
patients > 40 kg. encephalopathy), rash, hepatitis • If given with EFV: patients), dyslipidaemia (low
gynaecomastia ATV/r 400/100 mg potential), renal stones (rare) and
NVP 200 mg daily for 14 days and Rash, hepatitis daily hepatitis (uncommon)
then 200 mg 12 hourly LPV/r 400 mg/100 mg Gastrointestinal upset,
RPV 25 mg daily with food Rash, hepatitis, CNS symptoms (all 12 hourly or dyslipidaemia and hepatitis
800 mg/200 mg daily
uncommon) (only if PI-naïve)
ETR‡ 200 mg 12 hourly Rash and hepatitis (both uncommon) DRV/r 600 mg/100 mg Gastrointestinal upset, rash,
ADR, adverse drug reaction; CNS, central nervous system; EFV, efavirenz; ETR, etravirine; 12 hourly dyslipidaemia, hepatitis
NNRTI, non-nucleoside reverse transcriptase inhibitors; NVP, nevirapine; RPV, rilpivirine. 800 mg/100 mg daily (uncommon). Contains
†, Life-threatening reactions are indicated in bold. (only if no DRV sulphonamide moiety (use with
mutations)
caution in patients with sulpha
‡, NNRTI combinations to be avoided include (1) ETR + ATV/r (because of drug interaction) Consider 400 mg/100 mg allergy)
and (2) ETR + DTG unless a boosted PI is also used in the combination (because of drug daily (only if no
interaction). DRV mutations)
ADR, adverse drug reaction; ATV/r, atazanavir/ritonavir; DRV/r, darunavir/ritonavir; EFV,
blistering, then the NNRTI should be discontinued immediately efavirenz; LPV/r, lopinavir/ritonavir; PI, protease inhibitor.
and re-challenge must not be performed as these are features of †, Avoid the combination of ETR + ATV/r (because of drug interaction).
life-threatening reactions. If the rash is mild and occurs without Ritonavir is a PI in its own right, but is used principally as a
these features, then the NNRTI can be continued and the rash pharmacokinetic ‘booster’. As a potent inhibitor of CYP3A4, its
can be treated symptomatically with antihistamines and use results in higher drug levels and prolonged half-lives of its
possibly topical steroids. Systemic steroids should not be used. companion PI. This allows for lower or less frequent PI dosing
If there is a severe reaction to EFV or NVP, then we do not and decreases the chances of developing viral resistance. In rare
recommend switching to RPV or ETR – rather use DTG or a PI.
situations, ATV is used without boosting in first-line therapy.
However, this inhibition of CYP3A4, together with several
Dosage and common ADRs of NNRTIs available in southern other cytochrome P450 (CYP) enzymes and p-glycoprotein,
Africa are described in Table 5.
results in numerous drug–drug interactions with other
° Common pitfall: Immediately discontinuing NNRTIs medications (see section 17).
in the case of a mild rash without systemic features.
° Common pitfall: Not using a drug interaction checker
Such rashes often resolve if treatment is continued, when prescribing PI-based ART with other
although close monitoring is required.
medications. Clinically relevant drug–drug interactions
5. Protease inhibitor class of are common with this class.
antiretroviral drugs All PIs may be associated with cardiac conduction
Key points abnormalities (especially PR interval prolongation). This
seldom results in clinically significant effects, but caution
ÿ Three PI combinations are recommended in southern should be taken when co-prescribing other drugs that cause
Africa: lopinavir (LPV), ATV or darunavir (DRV), each delayed cardiac conduction, such as macrolides or
given with low-dose ritonavir (RTV, indicated as /r) for bedaquiline. All PIs are, to some extent, associated with
pharmacokinetic boosting. metabolic side effects. Elevated triglycerides (TGs) and
ÿ Ritonavir-boosted lopinavir is the only PI combination elevated low-density lipoprotein cholesterol (LDL-C) are
that can be used with RIF-based TB treatment, but the class effects, although these side effects are more pronounced
31,32
dose of LPV/r must be doubled. with LPV/r than with other PI combinations.
ÿ Atazanavir and DRV offer a better side effect profile than
LPV. Dosing and common ADRs of PIs are presented in Table 6.
ÿ Darunavir has the highest barrier to resistance of any
drug in this class. Individual protease inhibitors
Lopinavir
Overview of protease inhibitors Lopinavir is co-formulated with ritonavir (e.g. Aluvia): In
general, this twice-daily regimen has greater gastrointestinal
Protease inhibitors are a class of agents that inhibit HIV’s (GI) side effects than other PI combinations, and is associated
protease enzyme, which is required to cleave HIV’s with a worse metabolic profile. Lopinavir is the only PI that
polyproteins into the final protein products that permit the can be used concurrently with RIF-based TB treatment;
production of infectious viral particles. Inhibition of this the LPV/r dose has to be doubled in this instance to
process results in immature, non-infectious virions. 800 mg/200 mg twice daily until 2 weeks after RIF has been
stopped (see section 18).
Three PI combinations are recommended for use in southern
Africa: LPV, ATV and DRV, each given with low-dose ° Common pitfall: Forgetting to double the dose of
ritonavir. LPV/r when starting RIF-based TB treatment.
http://www.sajhivmed.org.za 26 Open Access