
Page 29 - HIVMED_v21_i1.indb
P. 29
Page 3 of 39 Guideline
These goals are achieved by suppressing viral replication ÿ Zidovudine (AZT) should only be used in special
completely for as long as possible, using well-tolerated and circumstances as a first-line drug.
sustainable treatment undertaken with good adherence. With ÿ Tenofovir disoproxil fumarate can cause renal failure or a
+
prolonged viral suppression, the CD4 lymphocyte count renal-tubular wasting syndrome. Creatinine monitoring
usually increases, which is accompanied by a restoration of at regular intervals is recommended.
pathogen-specific immune function. For most patients, this ÿ Abacavir can cause a fatal hypersensitivity reaction in
results in a dramatic reduction in the risk of HIV-associated patients with HLA-B*5701. If feasible, this allele should
morbidity and mortality. In patients who start to receive ART be excluded prior to starting ABC, although it is very rare
with preserved CD4 counts, ART is able to prevent the in people of African descent.
+
decline in CD4 count observed in untreated patients and ÿ Zidovudine can cause anaemia and neutropenia, and
+
prevent clinical complications of HIV infection. It is still regular monitoring of haemoglobin (Hb) and neutrophil
unclear whether immune function ever returns to full counts is recommended for the first 6 months.
normality, although long-term cohorts have shown that Available nucleoside or nucleotide reverse
patients who adhere well to ART have a near-normal life transcriptase inhibitors
1
expectancy. Patient adherence to the ART regimen remains a
key focus and challenge. Nucleoside reverse transcriptase inhibitors and nucleotide
reverse transcriptase inhibitors (NtRTIs) work by acting as
nucleotide base analogues. Following incorporation into the
Stopping antiretroviral therapy deoxyribonucleic acid (DNA) chain by HIV’s reverse
Antiretroviral therapy should not be stopped unless there transcriptase enzyme, they block further chain elongation.
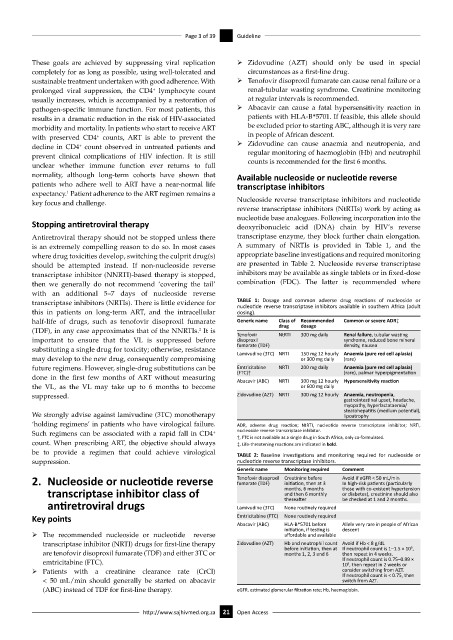
is an extremely compelling reason to do so. In most cases A summary of NRTIs is provided in Table 1, and the
where drug toxicities develop, switching the culprit drug(s) appropriate baseline investigations and required monitoring
should be attempted instead. If non-nucleoside reverse are presented in Table 2. Nucleoside reverse transcriptase
transcriptase inhibitor (NNRTI)-based therapy is stopped, inhibitors may be available as single tablets or in fixed-dose
then we generally do not recommend ‘covering the tail’ combination (FDC). The latter is recommended where
with an additional 5–7 days of nucleoside reverse
transcriptase inhibitors (NRTIs). There is little evidence for TABLE 1: Dosage and common adverse drug reactions of nucleoside or
nucleotide reverse transcriptase inhibitors available in southern Africa (adult
this in patients on long-term ART, and the intracellular dosing).
half-life of drugs, such as tenofovir disoproxil fumarate Generic name Class of Recommended Common or severe ADR‡
dosage
drug
(TDF), in any case approximates that of the NNRTIs. It is Tenofovir NtRTI 300 mg daily Renal failure, tubular wasting
2
important to ensure that the VL is suppressed before disoproxil syndrome, reduced bone mineral
substituting a single drug for toxicity; otherwise, resistance fumarate (TDF) density, nausea
may develop to the new drug, consequently compromising Lamivudine (3TC) NRTI 150 mg 12 hourly Anaemia (pure red cell aplasia)
or 300 mg daily
(rare)
future regimens. However, single-drug substitutions can be Emtricitabine NRTI 200 mg daily Anaemia (pure red cell aplasia)
(FTC)†
(rare), palmar hyperpigmentation
done in the first few months of ART without measuring Abacavir (ABC) NRTI 300 mg 12 hourly Hypersensitivity reaction
the VL, as the VL may take up to 6 months to become or 600 mg daily
suppressed. Zidovudine (AZT) NRTI 300 mg 12 hourly Anaemia, neutropenia,
gastrointestinal upset, headache,
myopathy, hyperlactataemia/
steatohepatitis (medium potential),
We strongly advise against lamivudine (3TC) monotherapy lipoatrophy
‘holding regimens’ in patients who have virological failure. ADR, adverse drug reaction; NtRTI, nucleotide reverse transcriptase inhibitor; NRTI,
+
Such regimens can be associated with a rapid fall in CD4 nucleoside reverse transcriptase inhibitor.
†, FTC is not available as a single drug in South Africa, only co-formulated.
count. When prescribing ART, the objective should always ‡, Life-threatening reactions are indicated in bold.
be to provide a regimen that could achieve virological TABLE 2: Baseline investigations and monitoring required for nucleoside or
suppression. nucleotide reverse transcriptase inhibitors.
Generic name Monitoring required Comment
2. Nucleoside or nucleotide reverse Tenofovir disoproxil Creatinine before Avoid if eGFR < 50 mL/min
fumarate (TDF)
initiation, then at 3
In high-risk patients (particularly
transcriptase inhibitor class of months, 6 months those with co-existent hypertension
or diabetes), creatinine should also
and then 6 monthly
antiretroviral drugs Lamivudine (3TC) thereafter be checked at 1 and 2 months.
None routinely required
Key points Emtricitabine (FTC) None routinely required
Abacavir (ABC) HLA-B*5701 before Allele very rare in people of African
initiation, if testing is descent
ÿ The recommended nucleoside or nucleotide reverse affordable and available
transcriptase inhibitor (NRTI) drugs for first-line therapy Zidovudine (AZT) Hb and neutrophil count Avoid if Hb < 8 g/dL 9
before initiation, then at If neutrophil count is 1–1.5 × 10 ,
are tenofovir disoproxil fumarate (TDF) and either 3TC or months 1, 2, 3 and 6 then repeat in 4 weeks.
emtricitabine (FTC). If neutrophil count is 0.75–0.99 ×
9
10 , then repeat in 2 weeks or
ÿ Patients with a creatinine clearance rate (CrCl) consider switching from AZT.
If neutrophil count is < 0.75, then
< 50 mL/min should generally be started on abacavir switch from AZT.
(ABC) instead of TDF for first-line therapy. eGFR, estimated glomerular filtration rate; Hb, haemoglobin.
http://www.sajhivmed.org.za 21 Open Access