
Page 365 - SAHCS HIVMed Journal Vol 20 No 1 2019
P. 365
Page 4 of 12 Original Research
Pregnancies/Deliveries Birth Outcomes
14 587 deliveries at PMMH
during study period
4170 deliveries not captured (weekend, public holiday and a er-hours
discharge; inaccessible records, including maternal deaths)
10 417 (71.4%) deliveries 10 517 birth outcomes including 98
captured pairs of twins and 1 set of triplets
6330 (60.2%) HIV 4063 (38.6%) HIV- 124 (1.2%) Birth
unexposed birth exposed birth outcomes with
outcomes outcomes unknown HIV exposure
3932 (96.8%) exposed to 131 (3.2%) not exposed
ART during pregnancy to ART during pregnancy
exclude 85 twin births and,
219 intrapartum regimen switches
3632 (89.4%) ART-exposed (2 twin deliveries also
birth outcomes included in had regimen switches)
risk analyses
380 (10.4%) definite 653 (18.0%) ambiguous 1494 (41.1%) post-T1 1105 (30.4%) unknown
and en re T1 exposure /par al T1 exposure exposure ming of exposure
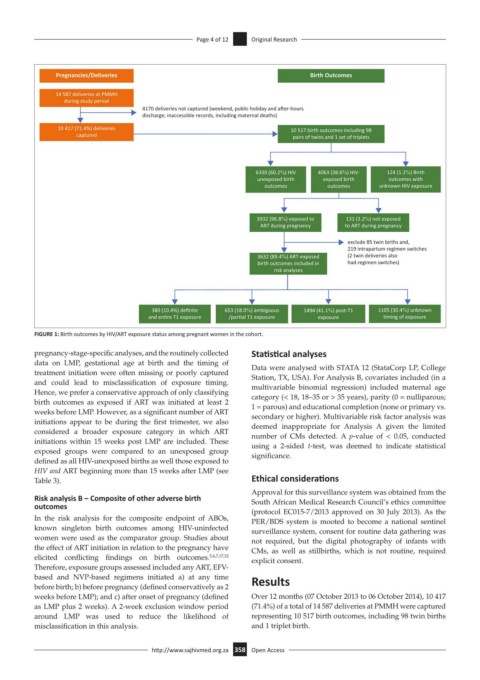
FIGURE 1: Birth outcomes by HIV/ART exposure status among pregnant women in the cohort.
pregnancy-stage-specific analyses, and the routinely collected Statistical analyses
data on LMP, gestational age at birth and the timing of Data were analysed with STATA 12 (StataCorp LP, College
treatment initiation were often missing or poorly captured Station, TX, USA). For Analysis B, covariates included (in a
and could lead to misclassification of exposure timing. multivariable binomial regression) included maternal age
Hence, we prefer a conservative approach of only classifying category (< 18, 18–35 or > 35 years), parity (0 = nulliparous;
birth outcomes as exposed if ART was initiated at least 2 1 = parous) and educational completion (none or primary vs.
weeks before LMP. However, as a significant number of ART secondary or higher). Multivariable risk factor analysis was
initiations appear to be during the first trimester, we also deemed inappropriate for Analysis A given the limited
considered a broader exposure category in which ART number of CMs detected. A p-value of < 0.05, conducted
initiations within 15 weeks post LMP are included. These using a 2-sided t-test, was deemed to indicate statistical
exposed groups were compared to an unexposed group significance.
defined as all HIV-unexposed births as well those exposed to
HIV and ART beginning more than 15 weeks after LMP (see
Table 3). Ethical considerations
Approval for this surveillance system was obtained from the
Risk analysis B – Composite of other adverse birth South African Medical Research Council’s ethics committee
outcomes
(protocol EC015-7/2013 approved on 30 July 2013). As the
In the risk analysis for the composite endpoint of ABOs, PER/BDS system is mooted to become a national sentinel
known singleton birth outcomes among HIV-uninfected surveillance system, consent for routine data gathering was
women were used as the comparator group. Studies about not required, but the digital photography of infants with
the effect of ART initiation in relation to the pregnancy have CMs, as well as stillbirths, which is not routine, required
elicited conflicting findings on birth outcomes. 5,6,7,17,32 explicit consent.
Therefore, exposure groups assessed included any ART, EFV-
based and NVP-based regimens initiated a) at any time Results
before birth; b) before pregnancy (defined conservatively as 2
weeks before LMP); and c) after onset of pregnancy (defined Over 12 months (07 October 2013 to 06 October 2014), 10 417
as LMP plus 2 weeks). A 2-week exclusion window period (71.4%) of a total of 14 587 deliveries at PMMH were captured
around LMP was used to reduce the likelihood of representing 10 517 birth outcomes, including 98 twin births
misclassification in this analysis. and 1 triplet birth.
http://www.sajhivmed.org.za 358 Open Access