
Page 31 - ONLINE – Nursing Matters October 2020_Vol 11
P. 31
MONITORING FOR ALL PATIENTS AT FIRST ANC VISIT clinical guidance
TB screening and sputum Gene Expert TB diagnosed: start TB Rx. If on ART, continue. If not yet on ART: see
$
(GXP) algorithm on centre spread PMTCT FOR MOTHERS 2019
To identify TB suspects and assess TPT TB excluded: start ART. If CD4 > 350, defer TPT until 6 weeks
eligibility postpartum. If CD4 ≤ 350, initiate TPT for 12 months
CrAg (cryptococcal antigen), If CrAg-positive: refer for urgent LP and patient should be discussed First version April 2020
if CD4 ≤ 100 with an expert. Fluconazole is teratogenic. Defer ART if ART-naïve, but
To treat or provide prophylaxis for don’t stop ART if already on ART
cryptococcal meningitis If CrAg-negative: start or continue ART RECOMMENDED REGIMENS
Screen for chronic diseases Treat according to relevant guidelines
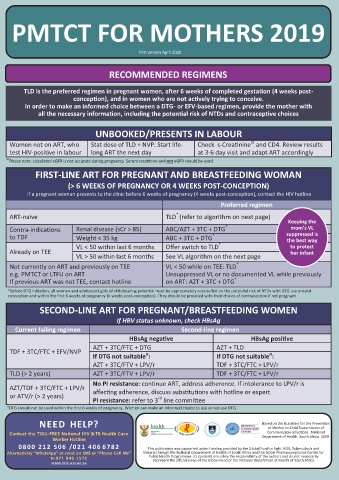
To identify high risk pregnancy TLD is the preferred regimen in pregnant women, after 6 weeks of completed gestation (4 weeks post-
Nutritional assessment All pregnant women should get calcium, folate and iron conception), and in women who are not actively trying to conceive.
To detect deficiency and provide necessary supplementation. Be aware that DTG interacts with some medicines: In order to make an informed choice between a DTG- or EFV-based regimen, provide the mother with
nutritional support refer to PMTCT guideline p17. Women with BMI < 23: refer to dietician all the necessary information, including the potential risk of NTDs and contraceptive choices
Family planning Provide counselling for safer sex, post-natal contraception and partner
testing UNBOOKED/PRESENTS IN LABOUR
STI and syphilis screening (RPR) If RPR done before 20 weeks and negative: repeat RPR at 32 weeks. Women not on ART, who Stat dose of TLD + NVP. Start life- Check s-Creatinine and CD4. Review results
ϖ
Treat all women with a positive syphilis screening test irrespective of
To identify and treat STIs test HIV-positive in labour long ART the next day at 3-6 day visit and adapt ART accordingly
titre: refer to PMTCT guideline p11
Viral load, if on ART See algorithm on centre spread. ϖ Please note: calculated eGFR is not accurate during pregnancy. Serum creatinine and not eGFR should be used
To identify treatment failure Be sure to check results and respond quickly! FIRST-LINE ART FOR PREGNANT AND BREASTFEEDING WOMAN
Hb or FBC Treat according to relevant guidelines
To detect anaemia and/or neutropaenia (> 6 WEEKS OF PREGNANCY OR 4 WEEKS POST-CONCEPTION)
Mental health screening Treat according to relevant guidelines If a pregnant woman presents to the clinic before 6 weeks of pregnancy (4 weeks post-conception), contact the HIV hotline
To identify mental health issues Preferred regimen
**
HBsAg , if unknown If HBsAg-positive: include TDF in regimen. Provide post-exposure
*
To assess HBV status prophylaxis of hepatitis B for infant as per relevant guidelines ART-naïve TLD (refer to algorithm on next page)
$ If the client has recently had TB, the GXP may give a false-positive. Please call an expert or the hotline to discuss; If HBsAg negative and not immune, provide Hep B Keeping the
**
mom’s VL
*
vaccination as per National Viral Hepatitis guidelines. Hep B vaccination is not contraindicated in pregnancy. If high-risk and status unknown at delivery, test. Contra-indications Renal disease (sCr > 85) ABC/AZT + 3TC + DTG suppressed is
*
MONITORING AT MONTHLY ANC VISITS: PATIENTS ON ART to TDF Weight < 35 kg ABC + 3TC + DTG * the best way
TEST AND PURPOSE TIMING AND RESPONSE Already on TEE VL < 50 within last 6 months Offer switch to TLD to protect
her infant
Viral load VL > 50 within last 6 months See VL algorithm on the next page
*
To confirm viral suppression or detect virological Refer to VL algorithm on previous page Not currently on ART and previously on TEE VL < 50 while on TEE: TLD
failure timeously e.g. PMTCT or LTFU on ART Unsuppressed VL or no documented VL while previously
*
CD4 count At 12 months on ART. Thereafter, repeat every 6 months until If previous ART was not TEE, contact hotline on ART: AZT + 3TC + DTG
client meets criteria to discontinue CPT
To assess immunological status, risk of OIs and Stop CD4 monitoring if client’s VL remains < 1000 c/mL. If VL > *Before DTG initiation, all women and adolescent girls of childbearing potential must be appropriately counselled on the potential risk of NTDs with DTG use around
conception and within the first 6 weeks of pregnancy (4 weeks post-conception). They should be provided with their choice of contraception if not pregnant
need for prophylaxis
1000 c/mL, monitor CD4 count every 6 months
TB symptom screening Every clinic visit SECOND-LINE ART FOR PREGNANT/BREASTFEEDING WOMEN
To identify TB suspects and assess TPT eligibility If HBV status unknown, check HBsAg
FBC, if on AZT At initiation, month 3, month 6, then annually Current failing regimen Second-line regimen
To detect anaemia and/or neutropaenia HBsAg negative HBsAg positive
ϖ
s-Creatinine , if on TDF At initiation, month 3, month 6, month 12 and then annually.
ϖ
To assess renal function and eligibility for TDF If s-Creatinine > 85 µmol/L: do not use TDF. See front page TDF + 3TC/FTC + EFV/NVP AZT + 3TC/FTC + DTG AZT + TLD
α
α
ϖ If DTG not suitable : If DTG not suitable :
Please note: calculated eGFR is not accurate during pregnancy. Serum creatinine and not eGFR should be used AZT + 3TC/FTV + LPV/r TDF + 3TC/FTC + LPV/r
BREASTFEEDING
• Breastfeeding should be initiated within one hour of delivery WHAT DOES TLD (> 2 years) AZT + 3TC/FTV + LPV/r TDF + 3TC/FTC + LPV/r
• Exclusive breastfeeding for first 6 months of life EXCLUSIVE No PI resistance: continue ART, address adherence. If intolerance to LPV/r is
• If mother is suppressed on ART, mixed feeding is not a reason to stop breastfeeding BREASTFEEDING MEAN? AZT/TDF + 3TC/FTC + LPV/r
• Introduction of age-appropriate solids from 6 months onwards For the first six months of or ATV/r (> 2 years) affecting adherence, discuss substitutions with hotline or expert
rd
• Continue breastfeeding until 2 years of age or older life, the baby only gets PI resistance: refer to 3 line committee
• Ensure mother is on ART, adherent and VL is suppressed mother’s milk and α DTG should not be used within the first 6 weeks of pregnancy. Women can make an informed choice to use or not use DTG
• It is recommended that women with a VL ≥ 1000 c/mL on first-line ART continue to breastfeed. Infant prophylaxis medication. This means no
should be extended/restarted while a concerted effort is made to re-suppress the mother’s VL water, formula, other foods
• Stopping breastfeeding should be done slowly, over a month or fluids Based on the Guideline for the Prevention
• Breastfeeding should be avoided in mothers who are failing second- or third-line NEED HELP? of Mother to Child Transmission of
Contact the TOLL-FREE National HIV & TB Health Care Communicable Infections . National
3TC = lamivudine; ABC = abacavir; ART = antiretroviral treatment; ATV/r = atazanavir/ritonavir; AZT = zidovudine; CPT = cotrimoxazole preventive therapy; CrAg = crypto- Worker Hotline Department of Health, South Africa. 2019.
coccal antigen; DTG = dolutegravir; EFV = efavirenz; FTC = emtricitabine; GXP = Gene Expert TB test; Hb = haemoglobin; HCT = HIV counselling and testing; HIV = human 0800 212 506 / 021 406 6782
immunodeficiency virus; IRIS = immune reconstitution syndrome; LP = lumbar puncture; LPV/r = lopinavir/ritonavir; MTCT = mother to child transfer; NTD = neural tube This publication was supported under funding provided by the Global Fund to Fight AIDS, Tuberculosis and
HIV Nursing Matters | October 2020 | page 28
HIV Nursing Matters | October 2020 | page 29
defect; NVP = nevirapine; OI = opportunistic infections; PCR = polymerase chain reaction; PICT = provider-initiated counselling and testing; PMTCT = prevention of mother Alternatively “WhatsApp” or send an SMS or “Please Call Me” Malaria through the National Department of Health of South Africa and the NDoH Pharmacovigilance Centre for
Public Health Programmes. Its contents are solely the responsibility of the authors and do not necessarily
to child transfer; LTFU = lost to follow-up; RTHB = road to health booklet; Rx = treatment; sCr = serum creatinine; STI = sexually transmitted infections; TDF = tenofovir; TEE to 071 840 1572 represent the official views of the Global Fund or the National Department of Health of South Africa
= tenofovir + emtricitabine + efavirenz; TLD = tenofovir + lamivudine + dolutegravir; TPT = tuberculosis preventive therapy; VL = viral load; WOCP = woman of childbearing www.mic.uct.ac.za
potential