
Page 184 - HIVMED_v21_i1.indb
P. 184
Page 3 of 6 Review Article
antibody-dependent cellular cytotoxicity of activated latently Furthermore, if the killing agent used in a hypothetical cure
36
infected cells in mice but human studies are required to is unable to penetrate the BBB, there would be no reduction
assess their efficacy. Killing agents that selectively induce in the size of the CNS reservoir. This makes the development
apoptosis of HIV-infected cells have also shown promise of a cure strategy distinct from ‘Shock and Kill’, involving the
in vitro (see Pro-apoptotic drugs [PADs]). direct killing of latent cells without the need for latency
reversal, desirable. The PAD class mentioned earlier has
Limitations of latency-reversing shown promise in achieving this.
agents Interactions of human
Whilst it has been repeatedly shown that LRAs alone are immunodeficiency virus with
unable to reduce the size of the latent HIV reservoir,
administration of a killing agent alongside an LRA has been apoptosis
37
proposed as a method of clearing the reactivated cells. The human immunodeficiency virus has complex
However, it seems likely that even with killing agents LRAs interactions with apoptosis pathways in infected cells.
40
cannot clear enough latent cells to achieve a functional cure In latently infected cells the increase in longevity observed
and may cause complications due to non-T cell HIV is partially the result of avoidance of apoptosis. A number
37
reservoirs. Future studies in humans to test the efficacy of of specific effects on apoptosis pathways have been
killing agents administrated alongside LRAs could be suggested as the cause of this. The intrinsic apoptosis
carried out by administering a previously tested LRA, such pathway is a response to cellular damage and involves
as disulfiram, alongside a killing agent such as a bNAb to pro-apoptotic factors causing mitochondrial outer membrane
participants living with HIV and measuring the change in permeabilisation (MOMP), triggering the release of soluble
38
reservoir size using a technique such as TILDA. However, proteins from the mitochondrial intermembrane space.
the combination of an LRA with, for example, a bNAb, is These include the cytochrome c and second mitochondria-
unlikely to clear the myeloid reservoir as dendritic cells are derived activator of caspase (SMAC, also known as
likely to be unaffected by LRAs. Therefore, even if DIABLO ). Cytochrome c binds cytosolic proteins to form
41
30
functional elimination of the T reservoir is achieved, viral the apoptosome, which activates the ‘initiator’ enzyme
CM
rebound on cART cessation may still occur due to the caspase-9. This, in turn, cleaves the ‘executioner’ enzymes
presence of the myeloid reservoir, which would likely not caspase-3 and caspase-7 which trigger the cleavage cascade
be cleared by current ‘Shock and Kill’ approaches under of other caspase enzymes resulting in cell death. The second
investigation. mitochondria-derived activator of caspase activates this
process through disinhibition of caspases 3, 7 and 9 via
Human immunodeficiency virus-associated neurological binding and inactivating the X-linked inhibitor of apoptosis
disorders (HANDs) are well-observed in patients on cART (XIAP). The X-linked inhibitor of apoptosis binds these
39
and may lead to widespread neurological impairment, caspases in the absence of SMAC, inhibiting their activity
suggesting significant damage to the CNS even when
viraemia elsewhere is suppressed below detectable levels. An retroviral drug LRA Viral protein
The cause of this appears to be relatively poor blood-brain HIV virion Inflammatory CK Viral protein
barrier (BBB) penetrance by antiretrovirals, allowing Neurotoxin
31
continued HIV replication alongside the presence of latently
infected microglial cells, perivascular macrophages and Neuron
astrocytes. Recent research suggests that impaired Microglial
20
neurogenesis may underpin HAND persistence even with cell 3
32
33
cART. A study on the CNS penetrance of LRAs showed
that disulfiram and vorinostat are able to cross the BBB Tissue B Cerebral
relatively easily. Whilst this could enable targeting of the macrophage B B vessel
CNS latent reservoir, it may mean that current in vivo
studies of LRAs are damaging to the patients involved, as
there is no reduction in latent reservoir size, whilst LRAs are 2
able to penetrate the CNS and increase viral replication with Astrocyte
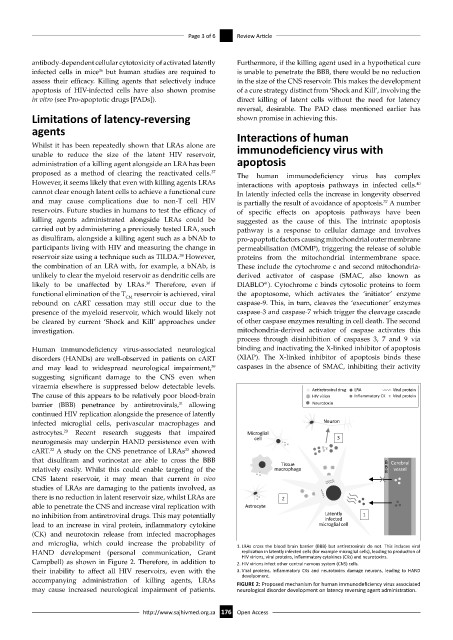
no inhibition from antiretroviral drugs. This may potentially Latently 1
infected
lead to an increase in viral protein, inflammatory cytokine microglial cell
(CK) and neurotoxin release from infected macrophages
and microglia, which could increase the probability of 1. LRAs cross the blood brain barrier (BBB) but antiretrovirals do not. This induces viral
HAND development (personal communication, Grant replication in latently infected cells (for example microglial cells), leading to production of
HIV virions, viral proteins, inflammatory cytokines (CKs) and neurotoxins.
Campbell) as shown in Figure 2. Therefore, in addition to 2. HIV virions infect other central nervous system (CNS) cells.
their inability to affect all HIV reservoirs, even with the 3. Viral proteins, inflammatory CKs and neurotoxins damage neurons, leading to HAND
develpoment.
accompanying administration of killing agents, LRAs FIGURE 2: Proposed mechanism for human immunodeficiency virus associated
may cause increased neurological impairment of patients. neurological disorder development on latency reversing agent administration.
http://www.sajhivmed.org.za 176 Open Access