
Page 160 - HIVMED_v21_i1.indb
P. 160
Page 7 of 9 Original Research
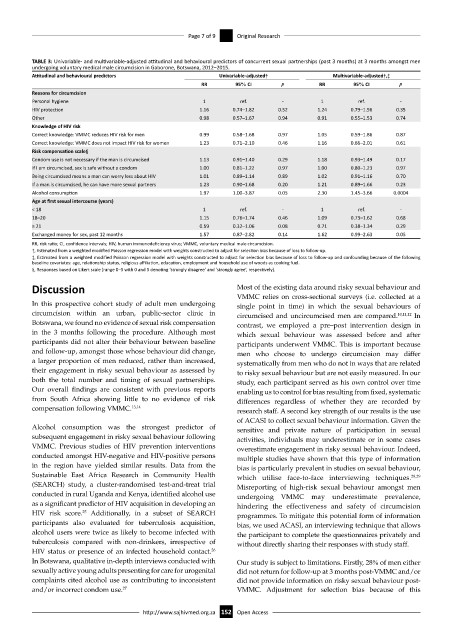
TABLE 3: Univariable- and multivariable-adjusted attitudinal and behavioural predictors of concurrent sexual partnerships (past 3 months) at 3 months amongst men
undergoing voluntary medical male circumcision in Gaborone, Botswana, 2012–2015.
Attitudinal and behavioural predictors Univariable-adjusted† Multivariable-adjusted†,‡
RR 95% CI p RR 95% CI p
Reasons for circumcision
Personal hygiene 1 ref. - 1 ref. -
HIV protection 1.16 0.74–1.82 0.52 1.24 0.79–1.96 0.35
Other 0.98 0.57–1.67 0.94 0.91 0.55–1.53 0.74
Knowledge of HIV risk
Correct knowledge: VMMC reduces HIV risk for men 0.99 0.58–1.68 0.97 1.05 0.59–1.86 0.87
Correct knowledge: VMMC does not impact HIV risk for women 1.23 0.71–2.10 0.46 1.16 0.66–2.01 0.61
Risk compensation scale§
Condom use is not necessary if the man is circumcised 1.13 0.91–1.40 0.29 1.18 0.93–1.49 0.17
If I am circumcised, sex is safe without a condom 1.00 0.81–1.22 0.97 1.00 0.80–1.23 0.97
Being circumcised means a man can worry less about HIV 1.01 0.89–1.14 0.89 1.02 0.91–1.16 0.70
If a man is circumcised, he can have more sexual partners 1.23 0.90–1.68 0.20 1.21 0.89–1.66 0.23
Alcohol consumption 1.97 1.00–3.87 0.05 2.30 1.45–3.66 0.0004
Age at first sexual intercourse (years)
< 18 1 ref. - 1 ref. -
18–20 1.15 0.76–1.74 0.46 1.09 0.73–1.62 0.68
≥ 21 0.59 0.32–1.06 0.08 0.71 0.38–1.34 0.29
Exchanged money for sex, past 12 months 1.57 0.87–2.82 0.14 1.62 0.99–2.63 0.05
RR, risk ratio; CI, confidence intervals; HIV, human immunodeficiency virus; VMMC, voluntary medical male circumcision.
†, Estimated from a weighted modified Poisson regression model with weights constructed to adjust for selection bias because of loss to follow-up.
‡, Estimated from a weighted modified Poisson regression model with weights constructed to adjust for selection bias because of loss to follow-up and confounding because of the following
baseline covariates: age, relationship status, religious affiliation, education, employment and household use of woods as cooking fuel.
§, Responses based on Likert scale (range 0–5 with 0 and 5 denoting ‘strongly disagree’ and ‘strongly agree’, respectively).
Discussion Most of the existing data around risky sexual behaviour and
VMMC relies on cross-sectional surveys (i.e. collected at a
In this prospective cohort study of adult men undergoing single point in time) in which the sexual behaviours of
circumcision within an urban, public-sector clinic in circumcised and uncircumcised men are compared. 10,11,12 In
Botswana, we found no evidence of sexual risk compensation contrast, we employed a pre–post intervention design in
in the 3 months following the procedure. Although most which sexual behaviour was assessed before and after
participants did not alter their behaviour between baseline participants underwent VMMC. This is important because
and follow-up, amongst those whose behaviour did change, men who choose to undergo circumcision may differ
a larger proportion of men reduced, rather than increased, systematically from men who do not in ways that are related
their engagement in risky sexual behaviour as assessed by to risky sexual behaviour but are not easily measured. In our
both the total number and timing of sexual partnerships. study, each participant served as his own control over time
Our overall findings are consistent with previous reports enabling us to control for bias resulting from fixed, systematic
from South Africa showing little to no evidence of risk differences regardless of whether they are recorded by
compensation following VMMC. 13,14 research staff. A second key strength of our results is the use
of ACASI to collect sexual behaviour information. Given the
Alcohol consumption was the strongest predictor of sensitive and private nature of participation in sexual
subsequent engagement in risky sexual behaviour following activities, individuals may underestimate or in some cases
VMMC. Previous studies of HIV prevention interventions overestimate engagement in risky sexual behaviour. Indeed,
conducted amongst HIV-negative and HIV-positive persons multiple studies have shown that this type of information
in the region have yielded similar results. Data from the bias is particularly prevalent in studies on sexual behaviour,
Sustainable East Africa Research in Community Health which utilise face-to-face interviewing techniques. 28,29
(SEARCH) study, a cluster-randomised test-and-treat trial Misreporting of high-risk sexual behaviour amongst men
conducted in rural Uganda and Kenya, identified alcohol use undergoing VMMC may underestimate prevalence,
as a significant predictor of HIV acquisition in developing an hindering the effectiveness and safety of circumcision
HIV risk score. Additionally, in a subset of SEARCH programmes. To mitigate this potential form of information
25
participants also evaluated for tuberculosis acquisition, bias, we used ACASI, an interviewing technique that allows
alcohol users were twice as likely to become infected with the participant to complete the questionnaires privately and
tuberculosis compared with non-drinkers, irrespective of without directly sharing their responses with study staff.
HIV status or presence of an infected household contact.
26
In Botswana, qualitative in-depth interviews conducted with Our study is subject to limitations. Firstly, 28% of men either
sexually active young adults presenting for care for urogenital did not return for follow-up at 3 months post-VMMC and/or
complaints cited alcohol use as contributing to inconsistent did not provide information on risky sexual behaviour post-
and/or incorrect condom use. 27 VMMC. Adjustment for selection bias because of this
http://www.sajhivmed.org.za 152 Open Access