
Page 155 - HIVMED_v21_i1.indb
P. 155
Page 2 of 9 Original Research
by circumcision. This phenomenon, known as risk Study setting and participants
compensation or behaviour disinhibition, may reduce the Adult men undergoing VMMC through the National Safe
effectiveness of VMMC in preventing new HIV infections. Male Circumcision programme were enrolled between
Although RCTs conducted in Kenya and Uganda indicated
that risk compensation behaviour did not increase following November 2013 and April 2015 at two government-run
9
circumcision, a RCT conducted in South Africa documented clinics providing free circumcision services in Gaborone,
a higher number of sexual contacts amongst circumcised the capital city of Botswana. Participant eligibility criteria
men compared with uncircumcised men in the control included: age ranging 18–49 years, residence within 25 km
group. However, amongst recent cross-sectional surveys of Gaborone, ever had sexual intercourse and documented
1
conducted in South Africa, Uganda and Kenya, there was no HIV-negative test result. All participants provided written
evidence that circumcised men’s behaviour was riskier than informed consent for participation in the study in addition
uncircumcised men’s behaviour. 10,11,12 to the consent obtained by clinic staff for the circumcision
procedure.
Men circumcised in non-clinical trial settings may also
encounter different experiences and behave differently. Sample size
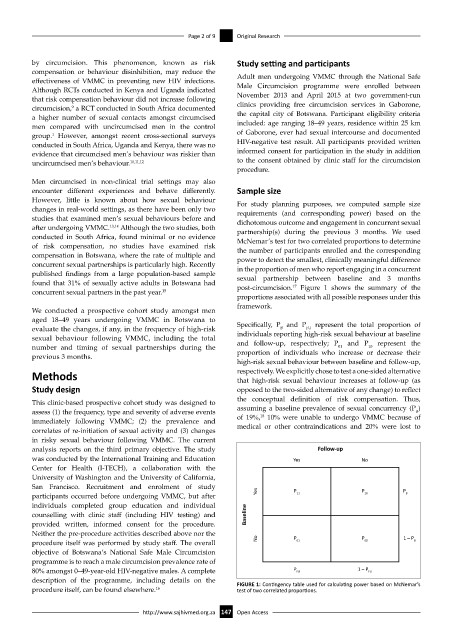
However, little is known about how sexual behaviour For study planning purposes, we computed sample size
changes in real-world settings, as there have been only two requirements (and corresponding power) based on the
studies that examined men’s sexual behaviours before and dichotomous outcome and engagement in concurrent sexual
after undergoing VMMC. 13,14 Although the two studies, both partnership(s) during the previous 3 months. We used
conducted in South Africa, found minimal or no evidence McNemar’s test for two correlated proportions to determine
of risk compensation, no studies have examined risk the number of participants enrolled and the corresponding
compensation in Botswana, where the rate of multiple and power to detect the smallest, clinically meaningful difference
concurrent sexual partnerships is particularly high. Recently in the proportion of men who report engaging in a concurrent
published findings from a large population-based sample sexual partnership between baseline and 3 months
found that 31% of sexually active adults in Botswana had post-circumcision. Figure 1 shows the summary of the
17
concurrent sexual partners in the past year. 15
proportions associated with all possible responses under this
framework.
We conducted a prospective cohort study amongst men
aged 18–49 years undergoing VMMC in Botswana to
FU
B
evaluate the changes, if any, in the frequency of high-risk Specifically, P and P represent the total proportion of
individuals reporting high-risk sexual behaviour at baseline
sexual behaviour following VMMC, including the total and follow-up, respectively; P and P represent the
number and timing of sexual partnerships during the proportion of individuals who increase or decrease their
10
01
previous 3 months.
high-risk sexual behaviour between baseline and follow-up,
Methods respectively. We explicitly chose to test a one-sided alternative
that high-risk sexual behaviour increases at follow-up (as
Study design opposed to the two-sided alternative of any change) to reflect
the conceptual definition of risk compensation. Thus,
This clinic-based prospective cohort study was designed to
assess (1) the frequency, type and severity of adverse events assuming a baseline prevalence of sexual concurrency (P )
B
18
immediately following VMMC; (2) the prevalence and of 19%, 10% were unable to undergo VMMC because of
medical or other contraindications and 20% were lost to
correlates of re-initiation of sexual activity and (3) changes
in risky sexual behaviour following VMMC. The current
analysis reports on the third primary objective. The study Follow-up
was conducted by the International Training and Education Yes No
Center for Health (I-TECH), a collaboration with the
University of Washington and the University of California,
San Francisco. Recruitment and enrolment of study P P P
participants occurred before undergoing VMMC, but after Yes 11 10 B
individuals completed group education and individual
counselling with clinic staff (including HIV testing) and Baseline
provided written, informed consent for the procedure.
Neither the pre-procedure activities described above nor the P P 1 – P
procedure itself was performed by study staff. The overall No 01 00 B
objective of Botswana’s National Safe Male Circumcision
programme is to reach a male circumcision prevalence rate of
80% amongst 0–49-year-old HIV-negative males. A complete P FU 1 – P FU
description of the programme, including details on the FIGURE 1: Contingency table used for calculating power based on McNemar’s
procedure itself, can be found elsewhere. 16 test of two correlated proportions.
http://www.sajhivmed.org.za 147 Open Access