
Page 150 - HIVMED_v21_i1.indb
P. 150
Page 5 of 8 Original Research
demographic, clinical or behavioural characteristics were Discussion
predictive of worsening sexual function (Table 2); results
were very similar in models restricted to sexually active men In this longitudinal evaluation of the men who became
and when excluding hygiene/cleanliness from the domains circumcised within a programmatic VMMC setting in
included in the outcome (data not shown). Botswana, we found very high overall satisfaction with the
procedure at 3 months after VMMC accompanied by frequently
Satisfaction with voluntary medical male reported improvement in sexual function. Consistent with
circumcision procedure prior data from research settings, our implementation
evaluation found that nearly all (98%) men were at least
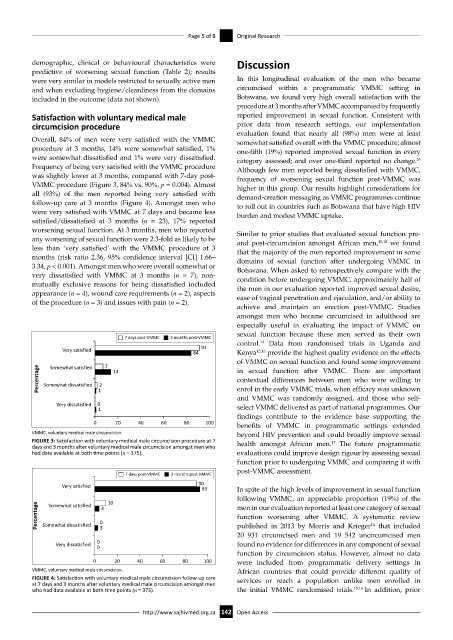
Overall, 84% of men were very satisfied with the VMMC somewhat satisfied overall with the VMMC procedure; almost
procedure at 3 months, 14% were somewhat satisfied, 1% one-fifth (19%) reported improved sexual function in every
were somewhat dissatisfied and 1% were very dissatisfied. category assessed; and over one-third reported no change.
26
Frequency of being very satisfied with the VMMC procedure Although few men reported being dissatisfied with VMMC,
was slightly lower at 3 months, compared with 7-day post- frequency of worsening sexual function post-VMMC was
VMMC procedure (Figure 3, 84% vs. 90%, p = 0.004). Almost higher in this group. Our results highlight considerations for
all (93%) of the men reported being very satisfied with demand-creation messaging as VMMC programmes continue
follow-up care at 3 months (Figure 4). Amongst men who to roll out in countries such as Botswana that have high HIV
were very satisfied with VMMC at 7 days and became less burden and modest VMMC uptake.
satisfied/dissatisfied at 3 months (n = 23), 17% reported
worsening sexual function. At 3 months, men who reported Similar to prior studies that evaluated sexual function pre-
any worsening of sexual function were 2.3-fold as likely to be and post-circumcision amongst African men, 15,18 we found
less than ‘very satisfied’ with the VMMC procedure at 3 that the majority of the men reported improvement in some
months (risk ratio 2.36, 95% confidence interval [CI] 1.66– domains of sexual function after undergoing VMMC in
3.34, p < 0.001). Amongst men who were overall somewhat or Botswana. When asked to retrospectively compare with the
very dissatisfied with VMMC at 3 months (n = 7), non- condition before undergoing VMMC, approximately half of
mutually exclusive reasons for being dissatisfied included the men in our evaluation reported improved sexual desire,
appearance (n = 4), wound care requirements (n = 2), aspects ease of vaginal penetration and ejaculation, and/or ability to
of the procedure (n = 3) and issues with pain (n = 2).
achieve and maintain an erection post-VMMC. Studies
amongst men who became circumcised in adulthood are
especially useful in evaluating the impact of VMMC on
sexual function because these men served as their own
7 days post-VMMC 3 months post-VMMC
control. Data from randomised trials in Uganda and
14
91
Very satisfied 84 Kenya 15,16 provide the highest quality evidence on the effects
of VMMC on sexual function and found some improvement
7
Somewhat satisfied
Percentage Somewhat dissatisfied 2 14 in sexual function after VMMC. There are important
contextual differences between men who were willing to
enrol in the early VMMC trials, when efficacy was unknown
1
and VMMC was randomly assigned, and those who self-
Very dissatisfied 0 select VMMC delivered as part of national programmes. Our
1
findings contribute to the evidence base supporting the
0 20 40 60 80 100
benefits of VMMC in programmatic settings extended
VMMC, voluntary medical male circumcision. beyond HIV prevention and could broadly improve sexual
FIGURE 3: Satisfaction with voluntary medical male circumcision procedure at 7 health amongst African men. The future programmatic
17
days and 3 months after voluntary medical male circumcision amongst men who
had data available at both time points (n = 375). evaluations could improve design rigour by assessing sexual
function prior to undergoing VMMC and comparing it with
post-VMMC assessment.
7 days post-VMMC 3 months post-VMMC
Very satisfied 90
93 In spite of the high levels of improvement in sexual function
following VMMC, an appreciable proportion (19%) of the
10 men in our evaluation reported at least one category of sexual
Somewhat satisfied
Percentage Somewhat dissatisfied 0 function worsening after VMMC. A systematic review
4
published in 2013 by Morris and Krieger that included
14
3
20 931 circumcised men and 19 542 uncircumcised men
0
Very dissatisfied found no evidence for differences in any component of sexual
0
function by circumcision status. However, almost no data
0 20 40 60 80 100 were included from programmatic delivery settings in
VMMC, voluntary medical male circumcision. African countries that could provide different quality of
FIGURE 4: Satisfaction with voluntary medical male circumcision follow-up care services or reach a population unlike men enrolled in
at 7 days and 3 months after voluntary medical male circumcision amongst men
who had data available at both time points (n = 375). the initial VMMC randomised trials. 15,16 In addition, prior
http://www.sajhivmed.org.za 142 Open Access