
Page 157 - HIVMED_v21_i1.indb
P. 157
Page 4 of 9 Original Research
provided a regression for participation is correctly specified
577
and no unobserved correlates of non-participation and risky Par cipants screened for
sexual behaviour exist. Inverse probability weights for eligibility* 14 Nov 2013 –
participation at follow-up were constructed from a 06 October 2015
multivariable logistic regression model, which considered the 22 (4%) Not sexually ac ve
following 24 potential covariates based on subject-matter 1 (< 1%) HIV-posi ve
knowledge: age, relationship status, religious affiliation,
education, employment status, household assets or 1 (< 1%) Aged < 18 years or > 49 years
27 (5%) Resided outside study area
characteristics, reason for circumcision, correct knowledge of (> 25 km from clinic)
circumcision benefits, beliefs about circumcision, alcohol use, 5 (1%) Not interested in study par cipa on
age at first sex, number of sexual partners (past 1 month, 523 (91%)
1 year and lifetime) and transactional sex. We also created 117 Eligible par cipants
enrolled in study
two-way interaction terms by taking the cross-product of each 4 (1%) Not circumcised due to medical
demographic and socioeconomic covariates with each contraindica ons and withdrawn from study
knowledge, belief and behavioural covariate. To build the 10 (2%) Refused baseline sexual behaviour
multivariate logistic regression model required by inverse- ques onnaire
509 (97%)
probability weighting, we used a stepwise, forward selection Circumcised par cipants
procedure to identify covariates from the list of candidate eligible for follow-up and
predictors listed above. The entry and exit criteria were set to completed baseline sexual
a p < 0.2. We included missing indicators for each selected behaviour ques onnaire
variable to maximise the number of cases included in the final 105 (21%)
Did not aend three month follow-up visit
models and to maintain a constant sample size across analyses.
36 (7%)
Aended three month follow-up visit
In post-hoc analyses, we sought to identify attitudes, beliefs 368 (72%) but refused sexual behaviour ques onnaire
and/or behaviours reported at baseline that may be Aened follow-up visit and
completed sexual
predictive of engagement (irrespective of what the participant behaviour ques onnaire
reported at baseline [i.e. pre-circumcision]) in high-risk at three months
sexual behaviour at 3 months post-VMMC. Specifically, we Note: *, Two particpants did not meet two eligibility vriteria. Therefore the number and
fit separate univariable- and multivariable-adjusted modified percentages presented for invidual reasons for ineligibility will sum to > 100%.
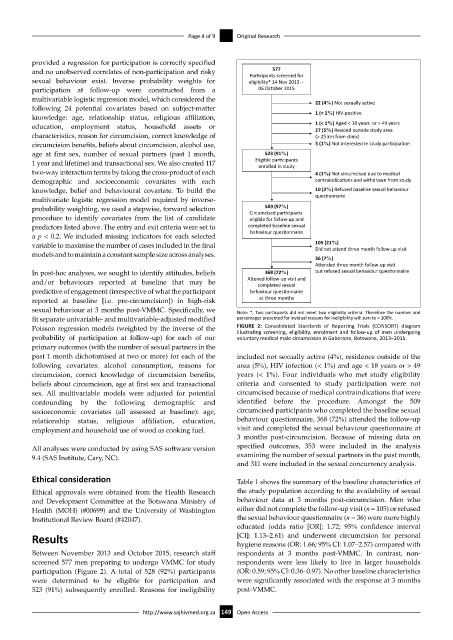
Poisson regression models (weighted by the inverse of the FIGURE 2: Consolidated Standards of Reporting Trials (CONSORT) diagram
illustrating screening, eligibility, enrolment and follow-up of men undergoing
probability of participation at follow-up) for each of our voluntary medical male circumcision in Gaborone, Botswana, 2013–2015.
primary outcomes (with the number of sexual partners in the
past 1 month dichotomised at two or more) for each of the included not sexually active (4%), residence outside of the
following covariates: alcohol consumption, reasons for area (5%), HIV infection (< 1%) and age < 18 years or > 49
circumcision, correct knowledge of circumcision benefits, years (< 1%). Four individuals who met study eligibility
beliefs about circumcision, age at first sex and transactional criteria and consented to study participation were not
sex. All multivariable models were adjusted for potential circumcised because of medical contraindications that were
confounding by the following demographic and identified before the procedure. Amongst the 509
socioeconomic covariates (all assessed at baseline): age, circumcised participants who completed the baseline sexual
relationship status, religious affiliation, education, behaviour questionnaire, 368 (72%) attended the follow-up
employment and household use of wood as cooking fuel. visit and completed the sexual behaviour questionnaire at
3 months post-circumcision. Because of missing data on
All analyses were conducted by using SAS software version specified outcomes, 353 were included in the analysis
9.4 (SAS Institute, Cary, NC). examining the number of sexual partners in the past month,
and 311 were included in the sexual concurrency analysis.
Ethical consideration Table 1 shows the summary of the baseline characteristics of
Ethical approvals were obtained from the Health Research the study population according to the availability of sexual
and Development Committee at the Botswana Ministry of behaviour data at 3 months post-circumcision. Men who
Health (MOH) (#00699) and the University of Washington either did not complete the follow-up visit (n = 105) or refused
Institutional Review Board (#42047). the sexual behaviour questionnaire (n = 36) were more highly
educated (odds ratio [OR]: 1.72; 95% confidence interval
Results [CI]: 1.13–2.61) and underwent circumcision for personal
hygiene reasons (OR: 1.66; 95% CI: 1.07–2.57) compared with
Between November 2013 and October 2015, research staff respondents at 3 months post-VMMC. In contrast, non-
screened 577 men preparing to undergo VMMC for study respondents were less likely to live in larger households
participation (Figure 2). A total of 528 (92%) participants (OR: 0.59; 95% CI: 0.36–0.97). No other baseline characteristics
were determined to be eligible for participation and were significantly associated with the response at 3 months
523 (91%) subsequently enrolled. Reasons for ineligibility post-VMMC.
http://www.sajhivmed.org.za 149 Open Access