
Page 216 - SAHCS HIVMed Journal Vol 20 No 1 2019
P. 216
Page 4 of 7 Original Research
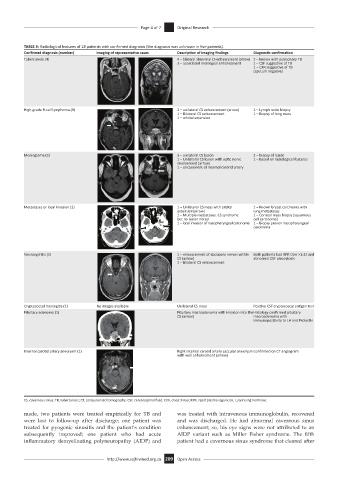
TABLE 3: Radiological features of 18 patients with confirmed diagnosis (the diagnosis was unknown in five patients).
Confirmed diagnosis (number) Imaging of representative cases Description of imaging findings Diagnostic confirmation
Tuberculosis (4) 4 – bilateral abnormal CS enhancement (arrow) 2 – known with pulmonary TB
3 – associated meningeal enhancement 1 – CSF suggestive of TB
1 – CXR suggestive of TB
(sputum negative)
High-grade B-cell lymphoma (3) 2 – unilateral CS enhancement (arrow) 2 – Lymph node biopsy
1 – Bilateral CS enhancement 1 – Biopsy of lung mass
1 – orbital extension
Meningioma (3) 3 – unilateral CS lesion 2 – biopsy of lesion
1 – Unilateral CS lesion with optic nerve 1 – Based on radiological features
involvement (arrow)
1 – encasement of Internal carotid artery
Metastases or local invasion (3) 1 – Unilateral CS mass with orbital 1 – Known breast carcinoma with
extension(arrow) lung metastases
1 – Multiple metastases. CS syndrome 1 – Corneal mass biopsy (squamous
but no lesion noted cell carcinoma)
1 – local invasion of nasopharyngeal carcinoma 1 – Biopsy proven nasopharyngeal
carcinoma
Neurosyphilis (2) 1 – enhancement of abducens nerves within Both patients had RPR titre >1:32 and
CS (arrow) abnormal CSF pleocytosis
1 – Bilateral CS enhancement
Cryptococcal meningitis (1) No images available Unilateral CS mass Positive CSF cryptococcal antigen test
Pituitary adenoma (1) Pituitary macroadenoma with invasion into the Histology confirmed pituitary
CS (arrow) macroadenoma with
immunopositivity to LH and Prolactin
Internal carotid artery aneurysm (1) Right internal carotid artery saccular aneurysm Confirmed on CT angiogram
with wall enhancement (arrow)
CS, cavernous sinus; TB, tuberculosis; CT, computerised tomography; CSF, cerebrospinal fluid; CXR, chest X-Ray; RPR, rapid plasma regain; LH, Luteinising hormone.
made, two patients were treated empirically for TB and was treated with intravenous immunoglobulin, recovered
were lost to follow-up after discharge; one patient was and was discharged. He had abnormal cavernous sinus
treated for pyogenic sinusitis and the patient’s condition enhancement; so, his eye signs were not attributed to an
subsequently improved; one patient who had acute AIDP variant such as Miller Fisher syndrome. The fifth
inflammatory demyelinating polyneuropathy (AIDP) and patient had a cavernous sinus syndrome that cleared after
http://www.sajhivmed.org.za 209 Open Access