
Page 57 - HIVMED_v21_i1.indb
P. 57
Page 31 of 39 Guideline
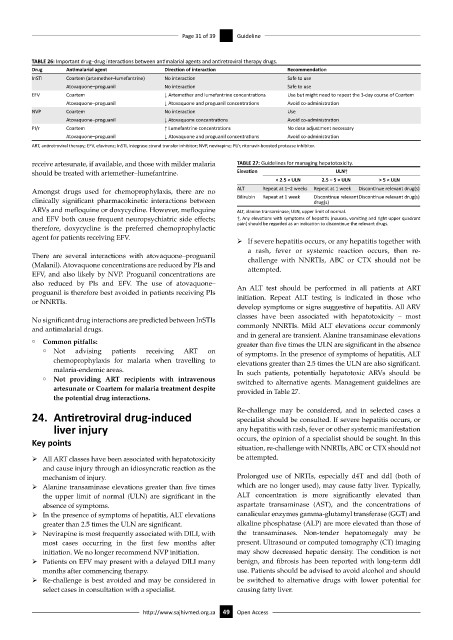
TABLE 26: Important drug–drug interactions between antimalarial agents and antiretroviral therapy drugs.
Drug Antimalarial agent Direction of interaction Recommendation
InSTI Coartem (artemether–lumefantrine) No interaction Safe to use
Atovaquone–proguanil No interaction Safe to use
EFV Coartem ↓ Artemether and lumefantrine concentrations Use but might need to repeat the 3-day course of Coartem
Atovaquone–proguanil ↓ Atovaquone and proguanil concentrations Avoid co-administration
NVP Coartem No interaction Use
Atovaquone–proguanil ↓ Atovaquone concentrations Avoid co-administration
PI/r Coartem ↑ Lumefantrine concentrations No dose adjustment necessary
Atovaquone–proguanil ↓ Atovaquone and proguanil concentrations Avoid co-administration
ART, antiretroviral therapy; EFV, efavirenz; InSTI, integrase strand transfer inhibitor; NVP, nevirapine; PI/r, ritonavir-boosted protease inhibitor.
receive artesunate, if available, and those with milder malaria TABLE 27: Guidelines for managing hepatotoxicity.
should be treated with artemether–lumefantrine. Elevation ULN†
< 2.5 × ULN 2.5 − 5 × ULN > 5 × ULN
Amongst drugs used for chemoprophylaxis, there are no ALT Repeat at 1–2 weeks Repeat at 1 week Discontinue relevant drug(s)
clinically significant pharmacokinetic interactions between Bilirubin Repeat at 1 week Discontinue relevant Discontinue relevant drug(s)
drug(s)
ARVs and mefloquine or doxycycline. However, mefloquine ALT, alanine transaminase; ULN, upper limit of normal.
and EFV both cause frequent neuropsychiatric side effects; †, Any elevations with symptoms of hepatitis (nausea, vomiting and right upper quadrant
therefore, doxycycline is the preferred chemoprophylactic pain) should be regarded as an indication to discontinue the relevant drugs.
agent for patients receiving EFV.
ÿ If severe hepatitis occurs, or any hepatitis together with
a rash, fever or systemic reaction occurs, then re-
There are several interactions with atovaquone–proguanil challenge with NNRTIs, ABC or CTX should not be
(Malanil). Atovaquone concentrations are reduced by PIs and attempted.
EFV, and also likely by NVP. Proguanil concentrations are
also reduced by PIs and EFV. The use of atovaquone– An ALT test should be performed in all patients at ART
proguanil is therefore best avoided in patients receiving PIs initiation. Repeat ALT testing is indicated in those who
or NNRTIs.
develop symptoms or signs suggestive of hepatitis. All ARV
classes have been associated with hepatotoxicity – most
No significant drug interactions are predicted between InSTIs
and antimalarial drugs. commonly NNRTIs. Mild ALT elevations occur commonly
and in general are transient. Alanine transaminase elevations
° Common pitfalls:
greater than five times the ULN are significant in the absence
° Not advising patients receiving ART on of symptoms. In the presence of symptoms of hepatitis, ALT
chemoprophylaxis for malaria when travelling to elevations greater than 2.5 times the ULN are also significant.
malaria-endemic areas. In such patients, potentially hepatotoxic ARVs should be
° Not providing ART recipients with intravenous
switched to alternative agents. Management guidelines are
artesunate or Coartem for malaria treatment despite provided in Table 27.
the potential drug interactions.
Re-challenge may be considered, and in selected cases a
24. Antiretroviral drug-induced specialist should be consulted. If severe hepatitis occurs, or
liver injury any hepatitis with rash, fever or other systemic manifestation
Key points occurs, the opinion of a specialist should be sought. In this
situation, re-challenge with NNRTIs, ABC or CTX should not
ÿ All ART classes have been associated with hepatotoxicity be attempted.
and cause injury through an idiosyncratic reaction as the
mechanism of injury. Prolonged use of NRTIs, especially d4T and ddI (both of
ÿ Alanine transaminase elevations greater than five times which are no longer used), may cause fatty liver. Typically,
the upper limit of normal (ULN) are significant in the ALT concentration is more significantly elevated than
absence of symptoms. aspartate transaminase (AST), and the concentrations of
ÿ In the presence of symptoms of hepatitis, ALT elevations canalicular enzymes gamma-glutamyl transferase (GGT) and
greater than 2.5 times the ULN are significant. alkaline phosphatase (ALP) are more elevated than those of
ÿ Nevirapine is most frequently associated with DILI, with the transaminases. Non-tender hepatomegaly may be
most cases occurring in the first few months after present. Ultrasound or computed tomography (CT) imaging
initiation. We no longer recommend NVP initiation. may show decreased hepatic density. The condition is not
ÿ Patients on EFV may present with a delayed DILI many benign, and fibrosis has been reported with long-term ddI
months after commencing therapy. use. Patients should be advised to avoid alcohol and should
ÿ Re-challenge is best avoided and may be considered in be switched to alternative drugs with lower potential for
select cases in consultation with a specialist. causing fatty liver.
http://www.sajhivmed.org.za 49 Open Access