
Page 334 - SAHCS HIVMed Journal Vol 20 No 1 2019
P. 334
Page 3 of 7 Original Research
TABLE 2: Maternal antiretroviral therapy, infant prophylaxis and feeding regimens recommended by the South African national prevention of mother-to-child transmission
programme of 2010 for human immunodeficiency virus-positive women during pregnancy and after delivery and their human immunodeficiency virus-exposed infants.
Variable PMTCT programme
2010 (1st edition) 19 2010 (2nd edition) 22
Maternal ART regimen
CD4 > 350 cells/mm 3 Dual therapy† Dual therapy†
CD4 ≤ 350 cells/mm or stage 3 or 4 HIV Lifelong cART‡ Lifelong cART‡
3
Infant prophylaxis
EFF NVP for 6 weeks NVP for 6 weeks
Breastfeeding without maternal lifelong cART NVP until 1 week post-cessation of breastfeeding NVP until 1 week post-cessation of breastfeeding
Breastfeeding with maternal lifelong cART NVP for 6 weeks NVP for 6 weeks
Infant feeding regimens EFF if the AFASS criteria are met Exclusive breastfeeding for all infants
Exclusive breastfeeding if AFASS criteria are not met
AFASS, acceptable, feasible, affordable, safe, sustainable; AZT, azidothymidine; cART, combination antiretroviral therapy; EFF, exclusive formula feeding; FTC, emtricitabine; NVP, nevirapine; TDF,
tenofovir.
†, Dual therapy: AZT from 14 weeks gestation, followed by three-hourly AZT and single dose NVP during labour, with a single dose of TDF and FTC after delivery (ART discontinued after delivery).
‡, Lifelong cART: TDF + lamivudine/FTC + NVP/efavirenz (continued after delivery).
Exclusion criteria
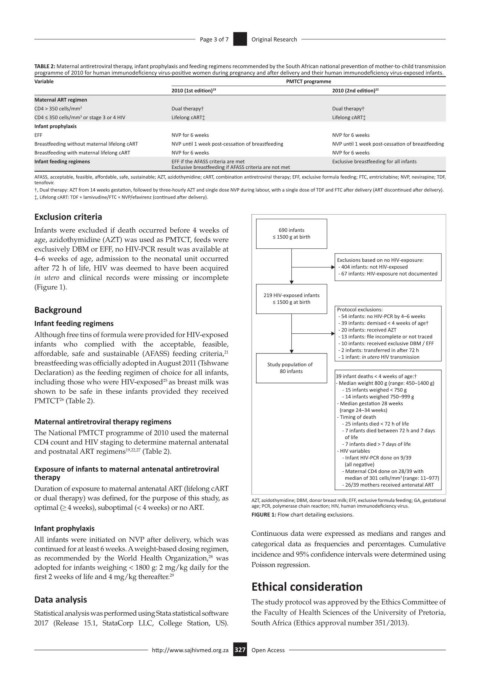
Infants were excluded if death occurred before 4 weeks of 690 infants
age, azidothymidine (AZT) was used as PMTCT, feeds were ≤ 1500 g at birth
exclusively DBM or EFF, no HIV-PCR result was available at
4–6 weeks of age, admission to the neonatal unit occurred Exclusions based on no HIV-exposure:
after 72 h of life, HIV was deemed to have been acquired - 404 infants: not HIV-exposed
in utero and clinical records were missing or incomplete - 67 infants: HIV-exposure not documented
(Figure 1).
219 HIV-exposed infants
≤ 1500 g at birth
Background Protocol exclusions:
- 54 infants: no HIV-PCR by 4–6 weeks
Infant feeding regimens - 39 infants: demised < 4 weeks of age†
- 20 infants: received AZT
Although free tins of formula were provided for HIV-exposed - 13 infants: file incomplete or not traced
infants who complied with the acceptable, feasible, - 10 infants: received exclusive DBM / EFF
affordable, safe and sustainable (AFASS) feeding criteria, - 2 infants: transferred in aer 72 h
21
- 1 infant: in utero HIV transmission
breastfeeding was officially adopted in August 2011 (Tshwane Study populaon of
Declaration) as the feeding regimen of choice for all infants, 80 infants 39 infant deaths < 4 weeks of age:†
including those who were HIV-exposed as breast milk was - Median weight 800 g (range: 450–1400 g)
25
shown to be safe in these infants provided they received - 15 infants weighed < 750 g
- 14 infants weighed 750–999 g
26
PMTCT (Table 2). - Median gestaon 28 weeks
(range 24–34 weeks)
Maternal antiretroviral therapy regimens - Timing of death
- 25 infants died < 72 h of life
The National PMTCT programme of 2010 used the maternal - 7 infants died between 72 h and 7 days
CD4 count and HIV staging to determine maternal antenatal of life
- 7 infants died > 7 days of life
and postnatal ART regimens 19,22,27 (Table 2). - HIV variables
- Infant HIV-PCR done on 9/39
(all negave)
Exposure of infants to maternal antenatal antiretroviral - Maternal CD4 done on 28/39 with
therapy median of 301 cells/mm (range: 11–977)
3
Duration of exposure to maternal antenatal ART (lifelong cART - 26/39 mothers received antenatal ART
or dual therapy) was defined, for the purpose of this study, as AZT, azidothymidine; DBM, donor breast milk; EFF, exclusive formula feeding; GA, gestational
optimal (≥ 4 weeks), suboptimal (< 4 weeks) or no ART. age; PCR, polymerase chain reaction; HIV, human immunodeficiency virus.
FIGURE 1: Flow chart detailing exclusions.
Infant prophylaxis Continuous data were expressed as medians and ranges and
All infants were initiated on NVP after delivery, which was categorical data as frequencies and percentages. Cumulative
continued for at least 6 weeks. A weight-based dosing regimen,
as recommended by the World Health Organization, was incidence and 95% confidence intervals were determined using
28
adopted for infants weighing < 1800 g: 2 mg/kg daily for the Poisson regression.
first 2 weeks of life and 4 mg/kg thereafter. 29
Ethical consideration
Data analysis The study protocol was approved by the Ethics Committee of
Statistical analysis was performed using Stata statistical software the Faculty of Health Sciences of the University of Pretoria,
2017 (Release 15.1, StataCorp LLC, College Station, US). South Africa (Ethics approval number 351/2013).
http://www.sajhivmed.org.za 327 Open Access