
Page 336 - SAHCS HIVMed Journal Vol 20 No 1 2019
P. 336
Page 5 of 7 Original Research
TABLE 4: Infant characteristics.
Clinical features All infants HIV-exposed HIV-infected
N = 80 (%) uninfected infants infants 79 infants
N = 78 (%) N = 2 (%)
n % n % n %
Pregnancy 80 - 78 - 2 - ART exposure Yes No Antenatal
Singleton 60 75.0 58 74.36 2 100 n = 63 n = 16
Multiple (twin) 20 25.0 20 25.64 - -
Gender 80 - 78 - 2 - prMOM n = 63 n = 16
Female 46 57.50 45 57.69 1 50.0 plus NVP Postnatal
Male 34 42.50 33 42.31 1 50.0
Mode of delivery 78 - 77 - 1 - HIV
Caesarean section 43 55.13 43 55.84 PCR Posi ve Nega ve Nega ve Posi ve
n = 14
n = 2
n = 63
n = 0
Vaginal delivery 30 38.46 29 37.66 1 100 result
BBA 5 6.41 5 6.49 - - prMOM plus NVP for 4–6 weeks prMOM plus NVP
(9 days and
Place of delivery 79 - 78 - 1 - 20 days)
Inborn 69 87.34 68 87.18 1 100
Outborn (including BBA) 10 12.66 10 12.82 - - ART, antiretroviral therapy; NVP, nevirapine; PCR, polymerase chain reaction; prMOM,
predominantly raw mother’s own milk; HIV, human immunodeficiency virus.
Amniotic membranes 49 - 49 - 0 - FIGURE 2: The safety of ‘raw’ mother’s own milk in human immunodeficiency
Intact 29 59.18 29 59.18 - - virus-exposed very low birth weight infants.
Ruptured < 24 h 9 18.37 9 18.37 - -
Ruptured ≥ 24 h† 11 22.45 11 22.45 - -
Placental histology 16 - 16 - 0 - Infants weighing ≤ 1500 g with HIV-PCR results
Acute chorioamnionitis 9 56.25 9 56.25 - - n = 80
Tuberculosis exposed 8 - 8 - 0 -
Received treatment 3 37.50 3 37.50
ART Posi ve HIV-PCR Nega ve HIV-PCR
Exposure to antenatal ART 80 - 78 - 2 - (> 72 h) by 4–6 weeks
Yes 63 78.75 63 80.77 - - n = 2 n = 78
No 16 20.0 14 17.95 2 100
Not documented 1 1.25 1 1.28 - - Scenario 1 Scenario 2 Scenario 3
Exposure to ≥ 4 weeks 49 - 49 - 0 -
antenatal ART In utero HIV infec on
Yes 37 75.51 37 75.51 - - In utero HIV infec on (n = 1) Peripartum Peripartum HIV
(n = 2)
(n = 2)
Lifelong cART 27 55.10 27 55.10 - - HIV (n = 1)
Dual therapy 10 20.41 10 20.41 - -
Exposure to postnatal 80 - 78 - 2 -
maternal cART Peripartum MTCT Peripartum MTCT Peripartum MTCT
Yes 40 50.0 40 51.28 - - 0% 1.27% 2.5%
No 39 48.75 37 47.44 2 100 (95% CI: 0) (95% CI: 0.2–8.9) (95% CI: 0.6–9.9)
Not documented 1 1.25 1 1.28 - -
Infant prophylaxis 80 - 78 - 2 - HIV, human immunodeficiency virus; PCR, polymerase chain reaction; MTCT, mother-to-child
Yes 80 100 78 100 2 100 HIV-transmission.
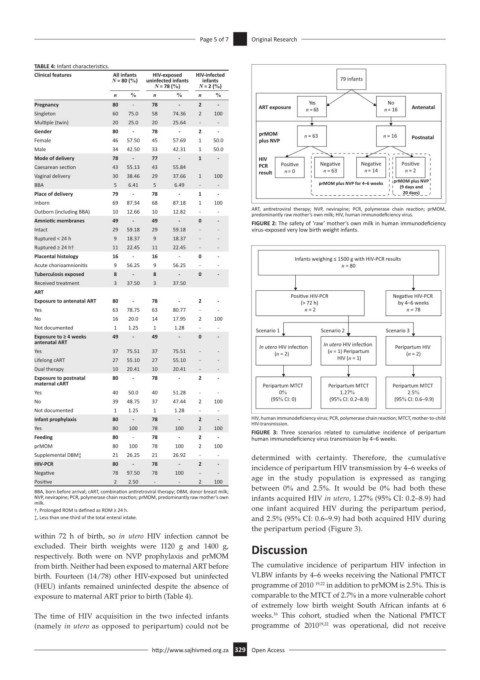
FIGURE 3: Three scenarios related to cumulative incidence of peripartum
Feeding 80 - 78 - 2 - human immunodeficiency virus transmission by 4–6 weeks.
prMOM 80 100 78 100 2 100
Supplemental DBM‡ 21 26.25 21 26.92 - - determined with certainty. Therefore, the cumulative
HIV-PCR 80 - 78 - 2 - incidence of peripartum HIV transmission by 4–6 weeks of
Negative 78 97.50 78 100 - -
Positive 2 2.50 - - 2 100 age in the study population is expressed as ranging
BBA, born before arrival; cART, combination antiretroviral therapy; DBM, donor breast milk; between 0% and 2.5%. It would be 0% had both these
NVP, nevirapine; PCR, polymerase chain reaction; prMOM, predominantly raw mother’s own infants acquired HIV in utero, 1.27% (95% CI: 0.2–8.9) had
milk.
†, Prolonged ROM is defined as ROM ≥ 24 h. one infant acquired HIV during the peripartum period,
‡, Less than one-third of the total enteral intake. and 2.5% (95% CI: 0.6–9.9) had both acquired HIV during
the peripartum period (Figure 3).
within 72 h of birth, so in utero HIV infection cannot be
excluded. Their birth weights were 1120 g and 1400 g, Discussion
respectively. Both were on NVP prophylaxis and prMOM
from birth. Neither had been exposed to maternal ART before The cumulative incidence of peripartum HIV infection in
birth. Fourteen (14/78) other HIV-exposed but uninfected VLBW infants by 4–6 weeks receiving the National PMTCT
(HEU) infants remained uninfected despite the absence of programme of 2010 19,22 in addition to prMOM is 2.5%. This is
exposure to maternal ART prior to birth (Table 4). comparable to the MTCT of 2.7% in a more vulnerable cohort
of extremely low birth weight South African infants at 6
16
The time of HIV acquisition in the two infected infants weeks. This cohort, studied when the National PMTCT
(namely in utero as opposed to peripartum) could not be programme of 2010 19,22 was operational, did not receive
http://www.sajhivmed.org.za 329 Open Access