
Page 281 - SAHCS HIVMed Journal Vol 20 No 1 2019
P. 281
Page 7 of 10 Original Research
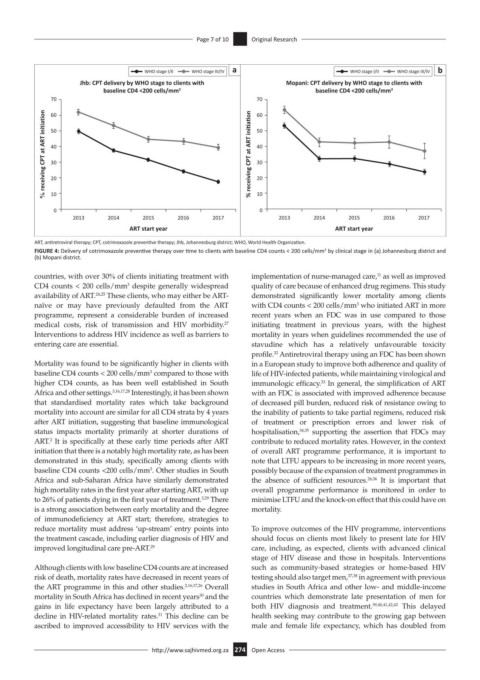
WHO stage I/II WHO stage III/IV a WHO stage I/II WHO stage III/IV b
Jhb: CPT delivery by WHO stage to clients with Mopani: CPT delivery by WHO stage to clients with
baseline CD4 <200 cells/mm 3 baseline CD4 <200 cells/mm 3
70 70
% receiving CPT at ART initiation 50 % receiving CPT at ART ini a on 50
60
60
40
40
30
30
20
20
10
0 10 0
2013 2014 2015 2016 2017 2013 2014 2015 2016 2017
ART start year ART start year
ART, antiretroviral therapy; CPT, cotrimoxazole preventive therapy; Jhb, Johannesburg district; WHO, World Health Organization.
FIGURE 4: Delivery of cotrimoxazole preventive therapy over time to clients with baseline CD4 counts < 200 cells/mm by clinical stage in (a) Johannesburg district and
3
(b) Mopani district.
countries, with over 30% of clients initiating treatment with implementation of nurse-managed care, as well as improved
11
CD4 counts < 200 cells/mm despite generally widespread quality of care because of enhanced drug regimens. This study
3
availability of ART. 24,25 These clients, who may either be ART- demonstrated significantly lower mortality among clients
naïve or may have previously defaulted from the ART with CD4 counts < 200 cells/mm who initiated ART in more
3
programme, represent a considerable burden of increased recent years when an FDC was in use compared to those
medical costs, risk of transmission and HIV morbidity. initiating treatment in previous years, with the highest
27
Interventions to address HIV incidence as well as barriers to mortality in years when guidelines recommended the use of
entering care are essential. stavudine which has a relatively unfavourable toxicity
profile. Antiretroviral therapy using an FDC has been shown
32
Mortality was found to be significantly higher in clients with in a European study to improve both adherence and quality of
baseline CD4 counts < 200 cells/mm compared to those with life of HIV-infected patients, while maintaining virological and
3
higher CD4 counts, as has been well established in South immunologic efficacy. In general, the simplification of ART
33
Africa and other settings. 3,16,17,28 Interestingly, it has been shown with an FDC is associated with improved adherence because
that standardised mortality rates which take background of decreased pill burden, reduced risk of resistance owing to
mortality into account are similar for all CD4 strata by 4 years the inability of patients to take partial regimens, reduced risk
after ART initiation, suggesting that baseline immunological of treatment or prescription errors and lower risk of
status impacts mortality primarily at shorter durations of hospitalisation, 34,35 supporting the assertion that FDCs may
2
ART. It is specifically at these early time periods after ART contribute to reduced mortality rates. However, in the context
initiation that there is a notably high mortality rate, as has been of overall ART programme performance, it is important to
demonstrated in this study, specifically among clients with note that LTFU appears to be increasing in more recent years,
3
baseline CD4 counts <200 cells/mm . Other studies in South possibly because of the expansion of treatment programmes in
Africa and sub-Saharan Africa have similarly demonstrated the absence of sufficient resources. 26,36 It is important that
high mortality rates in the first year after starting ART, with up overall programme performance is monitored in order to
to 26% of patients dying in the first year of treatment. There minimise LTFU and the knock-on effect that this could have on
3,29
is a strong association between early mortality and the degree mortality.
of immunodeficiency at ART start; therefore, strategies to
reduce mortality must address ‘up-stream’ entry points into To improve outcomes of the HIV programme, interventions
the treatment cascade, including earlier diagnosis of HIV and should focus on clients most likely to present late for HIV
improved longitudinal care pre-ART. 29 care, including, as expected, clients with advanced clinical
stage of HIV disease and those in hospitals. Interventions
Although clients with low baseline CD4 counts are at increased such as community-based strategies or home-based HIV
risk of death, mortality rates have decreased in recent years of testing should also target men, 37,38 in agreement with previous
the ART programme in this and other studies. 2,16,17,26 Overall studies in South Africa and other low- and middle-income
mortality in South Africa has declined in recent years and the countries which demonstrate late presentation of men for
30
gains in life expectancy have been largely attributed to a both HIV diagnosis and treatment. 39,40,41,42,43 This delayed
decline in HIV-related mortality rates. This decline can be health seeking may contribute to the growing gap between
31
ascribed to improved accessibility to HIV services with the male and female life expectancy, which has doubled from
http://www.sajhivmed.org.za 274 Open Access