
Page 268 - SAHCS HIVMed Journal Vol 20 No 1 2019
P. 268
Page 4 of 10 Original Research
Ethical consideration changed their NVP for EFV. In the TDF/FTC/RPV arm,
115/213 (54.0%) patients were taking an EFV-based regimen
Ethics committee approval was obtained at all participating and 98/213 (46.0%) patients were taking an NVP-based
centres in accordance with the principles of the 2008 regimen at screening. In the TDF/FTC/RPV arm, all (213
Declaration of Helsinki. [100.0%]) patients changed their NNRTI to RPV at
randomisation. In addition, all but two patients (99.1%) had a
Results switch in both their NNRTI and NRTI, while in the TDF/
Study patients FTC/EFV arm, only 45.5% had to switch both their NNRTI
and NRTI. In total, 397 (93.6%) of 424 patients stayed on
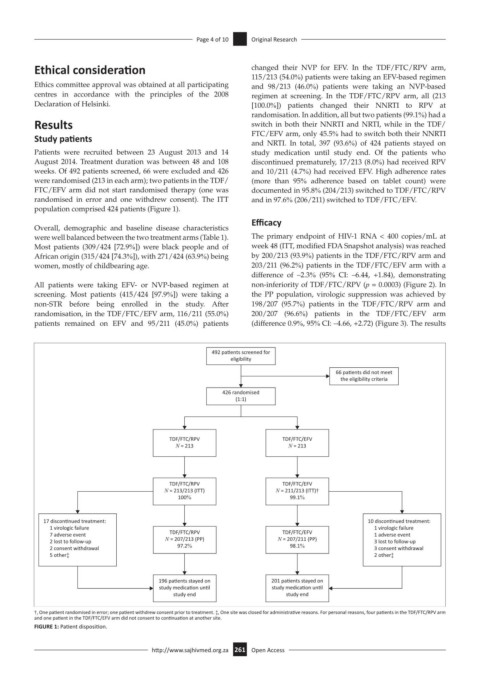
Patients were recruited between 23 August 2013 and 14 study medication until study end. Of the patients who
August 2014. Treatment duration was between 48 and 108 discontinued prematurely, 17/213 (8.0%) had received RPV
weeks. Of 492 patients screened, 66 were excluded and 426 and 10/211 (4.7%) had received EFV. High adherence rates
were randomised (213 in each arm); two patients in the TDF/ (more than 95% adherence based on tablet count) were
FTC/EFV arm did not start randomised therapy (one was documented in 95.8% (204/213) switched to TDF/FTC/RPV
randomised in error and one withdrew consent). The ITT and in 97.6% (206/211) switched to TDF/FTC/EFV.
population comprised 424 patients (Figure 1).
Efficacy
Overall, demographic and baseline disease characteristics
were well balanced between the two treatment arms (Table 1). The primary endpoint of HIV-1 RNA < 400 copies/mL at
Most patients (309/424 [72.9%]) were black people and of week 48 (ITT, modified FDA Snapshot analysis) was reached
African origin (315/424 [74.3%]), with 271/424 (63.9%) being by 200/213 (93.9%) patients in the TDF/FTC/RPV arm and
women, mostly of childbearing age. 203/211 (96.2%) patients in the TDF/FTC/EFV arm with a
difference of –2.3% (95% CI: –6.44, +1.84), demonstrating
All patients were taking EFV- or NVP-based regimen at non-inferiority of TDF/FTC/RPV (p = 0.0003) (Figure 2). In
screening. Most patients (415/424 [97.9%]) were taking a the PP population, virologic suppression was achieved by
non-STR before being enrolled in the study. After 198/207 (95.7%) patients in the TDF/FTC/RPV arm and
randomisation, in the TDF/FTC/EFV arm, 116/211 (55.0%) 200/207 (96.6%) patients in the TDF/FTC/EFV arm
patients remained on EFV and 95/211 (45.0%) patients (difference 0.9%, 95% CI: –4.66, +2.72) (Figure 3). The results
492 pa ents screened for
eligibility
66 pa ents did not meet
the eligibility criteria
426 randomised
(1:1)
TDF/FTC/RPV TDF/FTC/EFV
N = 213 N = 213
TDF/FTC/RPV TDF/FTC/EFV
N = 213/213 (ITT) N = 211/213 (ITT)†
100% 99.1%
17 discon nued treatment: 10 discon nued treatment:
1 virologic failure 1 virologic failure
7 adverse event TDF/FTC/RPV TDF/FTC/EFV 1 adverse event
2 lost to follow-up N = 207/213 (PP) N = 207/211 (PP) 3 lost to follow-up
2 consent withdrawal 97.2% 98.1% 3 consent withdrawal
5 other‡ 2 other‡
196 pa ents stayed on 201 pa ents stayed on
study medica on un l study medica on un l
study end study end
†, One patient randomised in error; one patient withdrew consent prior to treatment. ‡, One site was closed for administrative reasons. For personal reasons, four patients in the TDF/FTC/RPV arm
and one patient in the TDF/FTC/EFV arm did not consent to continuation at another site.
FIGURE 1: Patient disposition.
http://www.sajhivmed.org.za 261 Open Access