
Page 345 - HIVMED_v21_i1.indb
P. 345
Page 4 of 5 Original Research
16
adequately treated. Lumbar punctures and CSF drainage
50 No Yes
have been shown to be effective in managing CCM related
rIP. Alternatives such as acetazolamide or corticosteroids
17
Number of PLWHIV with CCM 30 44 38 instituted even when symptoms and signs of rIP are
have no role in the management of HIV/CCM.
18,19
40
Despite
the increased prevalence of rIP, therapeutic LPs are seldom
present.
In a clinical audit by Adeyemi and Ross, only 23%
13,16
of patients with CCM related headaches received therapeutic
20
LPs despite 82% of patients receiving analgesia for their
pain. Similarly, Rolfes et al. report that only 30% of the 248
13
patients in their cohort received therapeutic LPs. This was
14
10
18
despite the fact that therapeutic LPs were associated with a
5 69% improvement in survival. In our study we report a
14
0
Less than 4 LPs in the 4 or more LPs in 17.4% absolute risk reduction of in-hospital mortality
first 7 days the first 7 days following intervention with four or more LPs in the week of
Number of LPs received diagnosis and treatment.
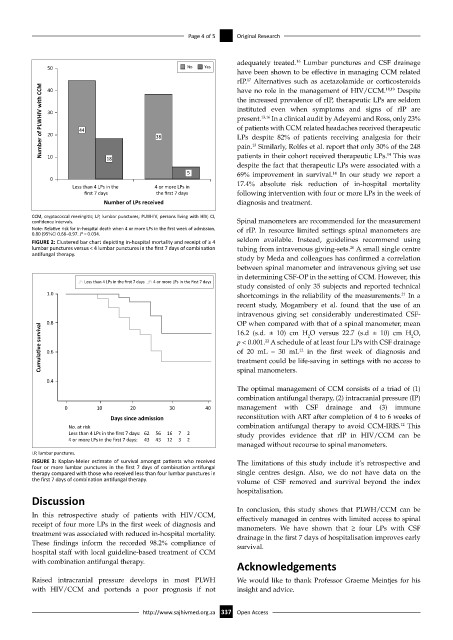
CCM, cryptococcal meningitis; LP, lumbar punctures; PLWHIV, persons living with HIV; CI,
confidence intervals. Spinal manometers are recommended for the measurement
Note: Relative risk for in-hospital death when 4 or more LPs in the first week of admission, of rIP. In resource limited settings spinal manometers are
0.80 (95%CI 0.66–0.97. P = 0.034.
FIGURE 2: Clustered bar chart depicting in-hospital mortality and receipt of ≥ 4 seldom available. Instead, guidelines recommend using
lumbar punctures versus < 4 lumbar punctures in the first 7 days of combination tubing from intravenous giving-sets. A small single centre
20
antifungal therapy.
study by Meda and colleagues has confirmed a correlation
between spinal manometer and intravenous giving set use
in determining CSF-OP in the setting of CCM. However, this
Less than 4 LPs in the first 7 days 4 or more LPs in the first 7 days
study consisted of only 35 subjects and reported technical
1.0 shortcomings in the reliability of the measurements. In a
21
recent study, Mogambery et al. found that the use of an
intravenous giving set considerably underestimated CSF-
0.8 OP when compared with that of a spinal manometer, mean
Cumula ve survival 0.6 p < 0.001. A schedule of at least four LPs with CSF drainage
16.2 (s.d. ± 10) cm H O versus 22.7 (s.d ± 10) cm H O,
2
2
22
of 20 mL – 30 mL in the first week of diagnosis and
12
treatment could be life-saving in settings with no access to
0.4 spinal manometers.
The optimal management of CCM consists of a triad of (1)
combination antifungal therapy, (2) intracranial pressure (IP)
0 10 20 30 40 management with CSF drainage and (3) immune
Days since admission reconstitution with ART after completion of 4 to 6 weeks of
12
No. at risk combination antifungal therapy to avoid CCM-IRIS. This
Less than 4 LPs in the first 7 days: 62 56 16 7 2 study provides evidence that rIP in HIV/CCM can be
4 or more LPs in the first 7 days: 43 43 12 3 2
managed without recourse to spinal manometers.
LP, lumbar punctures.
FIGURE 3: Kaplan-Meier estimate of survival amongst patients who received The limitations of this study include it’s retrospective and
four or more lumbar punctures in the first 7 days of combination antifungal
therapy compared with those who received less than four lumbar punctures in single centres design. Also, we do not have data on the
the first 7 days of combination antifungal therapy. volume of CSF removed and survival beyond the index
hospitalisation.
Discussion
In conclusion, this study shows that PLWH/CCM can be
In this retrospective study of patients with HIV/CCM, effectively managed in centres with limited access to spinal
receipt of four more LPs in the first week of diagnosis and manometers. We have shown that ≥ four LPs with CSF
treatment was associated with reduced in-hospital mortality. drainage in the first 7 days of hospitalisation improves early
These findings inform the recorded 98.2% compliance of survival.
hospital staff with local guideline-based treatment of CCM
with combination antifungal therapy.
Acknowledgements
Raised intracranial pressure develops in most PLWH We would like to thank Professor Graeme Meintjes for his
with HIV/CCM and portends a poor prognosis if not insight and advice.
http://www.sajhivmed.org.za 337 Open Access