
Page 215 - HIVMED_v21_i1.indb
P. 215
Page 6 of 9 Original Research
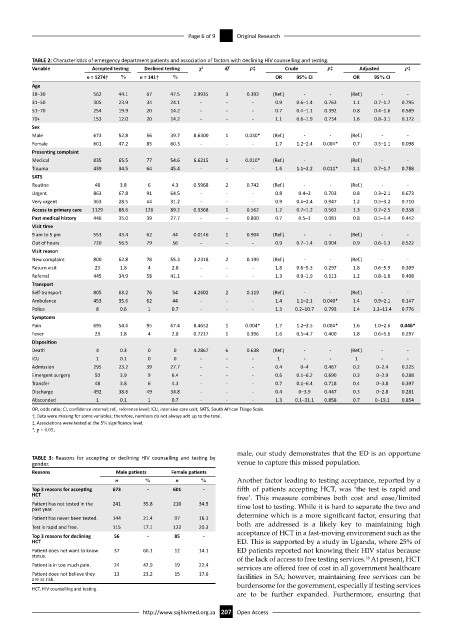
TABLE 2: Characteristics of emergency department patients and association of factors with declining HIV counselling and testing.
Variable Accepted testing Declined testing χ 2 df p‡ Crude p‡ Adjusted p‡
n = 1274† % n = 141† % OR 95% CI OR 95% CI
Age
18–30 562 44.1 67 47.5 2.9935 3 0.393 (Ref.) - - (Ref.) - -
31–50 305 23.9 34 24.1 - - - 0.9 0.6–1.4 0.763 1.1 0.7–1.7 0.795
51–70 254 19.9 20 14.2 - - - 0.7 0.4–1.1 0.392 0.8 0.4–1.6 0.589
70+ 153 12.0 20 14.2 - - - 1.1 0.6–1.9 0.734 1.6 0.8–3.1 0.172
Sex
Male 673 52.8 56 39.7 8.6300 1 0.030* (Ref.) - - (Ref.) - -
Female 601 47.2 85 60.3 - - - 1.7 1.2–2.4 0.004* 0.7 0.5–1.1 0.098
Presenting complaint
Medical 835 65.5 77 54.6 6.6215 1 0.010* (Ref.) - - (Ref.) - -
Trauma 439 34.5 64 45.4 - - - 1.6 1.1–2.2 0.011* 1.1 0.7–1.7 0.788
SATS
Routine 48 3.8 6 4.3 0.5968 2 0.742 (Ref.) - - (Ref.) - -
Urgent 863 67.8 91 64.5 - - - 0.8 0.4–2 0.703 0.8 0.3–2.1 0.673
Very urgent 363 28.5 44 31.2 - - - 0.9 0.4–2.4 0.947 1.2 0.5–3.2 0.710
Access to primary care 1129 88.6 126 89.2 0.3368 1 0.562 1.2 0.7–1.2 0.562 1.3 0.7–2.5 0.358
Past medical history 446 35.0 39 27.7 - - 0.800 0.7 0.5–1 0.081 0.8 0.5–1.4 0.442
Visit time
9 am to 5 pm 553 43.4 62 44 0.0146 1 0.904 (Ref.) - - (Ref.) - -
Out of hours 720 56.5 79 56 - - - 0.9 0.7–1.4 0.904 0.9 0.6–1.3 0.522
Visit reason
New complaint 800 62.8 78 55.3 3.2318 2 0.199 (Ref.) - - (Ref.) - -
Return visit 23 1.8 4 2.8 - - - 1.8 0.6–5.3 0.297 1.8 0.6–5.9 0.309
Referral 445 34.9 58 41.1 - - - 1.3 0.9–1.9 0.113 1.2 0.8–1.8 0.408
Transport
Self-transport 805 63.2 76 54 4.2602 2 0.119 (Ref.) - - (Ref.) - -
Ambulance 453 35.6 62 44 - - - 1.4 1.1–2.1 0.040* 1.4 0.9–2.1 0.147
Police 8 0.6 1 0.7 - - - 1.3 0.2–10.7 0.793 1.4 1.2–11.4 0.776
Symptoms
Pain 695 54.6 95 67.4 8.4652 1 0.004* 1.7 1.2–2.5 0.004* 1.6 1.0–2.6 0.046*
Fever 23 1.8 4 2.8 0.7217 1 0.396 1.6 0.5–4.7 0.400 1.8 0.6–5.6 0.297
Disposition
Death 4 0.3 0 0 4.2867 6 0.638 (Ref.) - - (Ref.) - -
ICU 1 0.1 0 0 - - - 1 - - 1 - -
Admission 295 23.2 39 27.7 - - - 0.4 0–4 0.467 0.2 0–2.4 0.225
Emergent surgery 50 3.9 9 6.4 - - - 0.6 0.1–6.2 0.690 0.3 0–2.9 0.288
Transfer 48 3.8 6 4.3 - - - 0.7 0.1–6.4 0.718 0.4 0–3.8 0.397
Discharge 492 38.6 49 34.8 - - - 0.4 0–3.9 0.447 0.3 0–2.8 0.281
Absconded 1 0.1 1 0.7 - - - 1.3 0.1–31.1 0.858 0.7 0–19.1 0.854
OR, odds ratio; CI, confidence interval; ref., reference level; ICU, intensive care unit; SATS, South African Triage Scale.
†, Data were missing for some variables; therefore, numbers do not always add up to the total.
‡, Associations were tested at the 5% significance level.
*, p < 0.05.,
male, our study demonstrates that the ED is an opportune
TABLE 3: Reasons for accepting or declining HIV counselling and testing by
gender. venue to capture this missed population.
Reasons Male patients Female patients
n % n % Another factor leading to testing acceptance, reported by a
Top 3 reasons for accepting 673 - 601 - fifth of patients accepting HCT, was ‘the test is rapid and
HCT free’. This measure combines both cost and ease/limited
Patient has not tested in the 241 35.8 210 34.9 time lost to testing. While it is hard to separate the two and
past year.
Patient has never been tested. 144 21.4 97 16.1 determine which is a more significant factor, ensuring that
both are addressed is a likely key to maintaining high
Test is rapid and free. 115 17.1 122 20.3
Top 3 reasons for declining 56 - 85 - acceptance of HCT in a fast-moving environment such as the
HCT ED. This is supported by a study in Uganda, where 25% of
Patient does not want to know 37 66.1 12 14.1 ED patients reported not knowing their HIV status because
status. of the lack of access to free testing services. At present, HCT
16
Patient is in too much pain. 24 42.9 19 22.4 services are offered free of cost in all government healthcare
Patient does not believe they 13 23.2 15 17.6 facilities in SA; however, maintaining free services can be
are at risk.
burdensome for the government, especially if testing services
HCT, HIV counselling and testing.
are to be further expanded. Furthermore, ensuring that
http://www.sajhivmed.org.za 207 Open Access