
Page 213 - HIVMED_v21_i1.indb
P. 213
Page 4 of 9 Original Research
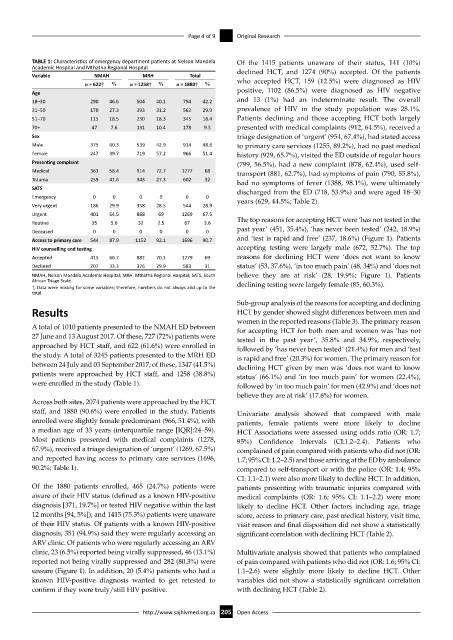
TABLE 1: Characteristics of emergency department patients at Nelson Mandela Of the 1415 patients unaware of their status, 141 (10%)
Academic Hospital and Mthatha Regional Hospital. declined HCT, and 1274 (90%) accepted. Of the patients
Variable NMAH MRH Total
n = 622† % n = 1258† % n = 1880† % who accepted HCT, 159 (12.5%) were diagnosed as HIV
Age positive, 1102 (86.5%) were diagnosed as HIV negative
18–30 290 46.6 504 40.1 794 42.2 and 13 (1%) had an indeterminate result. The overall
31–50 170 27.3 393 31.2 563 29.9 prevalence of HIV in the study population was 28.1%.
51–70 115 18.5 230 18.3 345 18.4 Patients declining and those accepting HCT both largely
70+ 47 7.6 131 10.4 178 9.5 presented with medical complaints (912, 64.5%), received a
Sex triage designation of ‘urgent’ (954, 67.4%), had stated access
Male 375 60.3 539 42.9 914 48.6 to primary care services (1255, 89.2%), had no past medical
Female 247 39.7 719 57.2 966 51.4 history (929, 65.7%), visited the ED outside of regular hours
Presenting complaint (799, 56.5%), had a new complaint (878, 62.4%), used self-
Medical 363 58.4 914 72.7 1277 68 transport (881, 62.7%), had symptoms of pain (790, 55.8%),
Trauma 259 41.6 343 27.3 602 32 had no symptoms of fever (1388, 98.1%), were ultimately
SATS discharged from the ED (718, 53.9%) and were aged 18–30
Emergency 0 0 0 0 0 0 years (629, 44.5%; Table 2).
Very urgent 186 29.9 358 28.5 544 28.9
Urgent 401 64.5 868 69 1269 67.5
Routine 35 5.6 32 2.5 67 3.6 The top reasons for accepting HCT were ‘has not tested in the
Deceased 0 0 0 0 0 0 past year’ (451, 35.4%), ‘has never been tested’ (242, 18.9%)
Access to primary care 544 87.9 1152 92.1 1696 90.7 and ‘test is rapid and free’ (237, 18.6%) (Figure 1). Patients
HIV counselling and testing accepting testing were largely male (672, 52.7%). The top
Accepted 415 66.7 882 70.1 1279 69 reasons for declining HCT were ‘does not want to know
Declined 207 33.3 376 29.9 583 31 status’ (53, 37.6%), ‘in too much pain’ (48, 34%) and ‘does not
NMAH, Nelson Mandela Academic Hospital; MRH, Mthatha Regional Hospital; SATS, South believe they are at risk’ (28, 19.9%; Figure 1). Patients
African Triage Scale. declining testing were largely female (85, 60.3%).
†, Data were missing for some variables; therefore, numbers do not always add up to the
total.
Sub-group analysis of the reasons for accepting and declining
Results HCT by gender showed slight differences between men and
women in the reported reasons (Table 3). The primary reason
A total of 1010 patients presented to the NMAH ED between for accepting HCT for both men and women was ‘has not
27 June and 13 August 2017. Of these, 727 (72%) patients were tested in the past year’, 35.8% and 34.9%, respectively,
approached by HCT staff, and 622 (61.6%) were enrolled in followed by ‘has never been tested’ (21.4%) for men and ‘test
the study. A total of 3245 patients presented to the MRH ED is rapid and free’ (20.3%) for women. The primary reason for
between 24 July and 03 September 2017; of these, 1347 (41.5%) declining HCT given by men was ‘does not want to know
patients were approached by HCT staff, and 1258 (38.8%) status’ (66.1%) and ‘in too much pain’ for women (22.4%),
were enrolled in the study (Table 1). followed by ‘in too much pain’ for men (42.9%) and ‘does not
believe they are at risk’ (17.6%) for women.
Across both sites, 2074 patients were approached by the HCT
staff, and 1880 (90.6%) were enrolled in the study. Patients Univariate analysis showed that compared with male
enrolled were slightly female predominant (966, 51.4%), with patients, female patients were more likely to decline
a median age of 33 years (interquartile range [IQR]:24–59). HCT Associations were assessed using odds ratio (OR: 1.7;
Most patients presented with medical complaints (1278, 95%) Confidence Intervals (CI:1.2–2.4). Patients who
67.9%), received a triage designation of ‘urgent’ (1269, 67.5%) complained of pain compared with patients who did not (OR:
and reported having access to primary care services (1696, 1.7; 95% CI: 1.2–2.5) and those arriving at the ED by ambulance
90.2%; Table 1). compared to self-transport or with the police (OR: 1.4; 95%
CI: 1.1–2.1) were also more likely to decline HCT. In addition,
Of the 1880 patients enrolled, 465 (24.7%) patients were patients presenting with traumatic injuries compared with
aware of their HIV status (defined as a known HIV-positive medical complaints (OR: 1.6; 95% CI: 1.1–2.2) were more
diagnosis [371, 19.7%] or tested HIV negative within the last likely to decline HCT. Other factors including age, triage
12 months [94, 5%]), and 1415 (75.3%) patients were unaware score, access to primary care, past medical history, visit time,
of their HIV status. Of patients with a known HIV-positive visit reason and final disposition did not show a statistically
diagnosis, 351 (94.9%) said they were regularly accessing an significant correlation with declining HCT (Table 2).
ARV clinic. Of patients who were regularly accessing an ARV
clinic, 23 (6.5%) reported being virally suppressed, 46 (13.1%) Multivariate analysis showed that patients who complained
reported not being virally suppressed and 282 (80.3%) were of pain compared with patients who did not (OR: 1.6; 95% CI:
unsure (Figure 1). In addition, 20 (5.4%) patients who had a 1.1–2.6) were slightly more likely to decline HCT. Other
known HIV-positive diagnosis wanted to get retested to variables did not show a statistically significant correlation
confirm if they were truly/still HIV positive. with declining HCT (Table 2).
http://www.sajhivmed.org.za 205 Open Access