
Page 167 - HIVMED_v21_i1.indb
P. 167
Page 5 of 8 Original Research
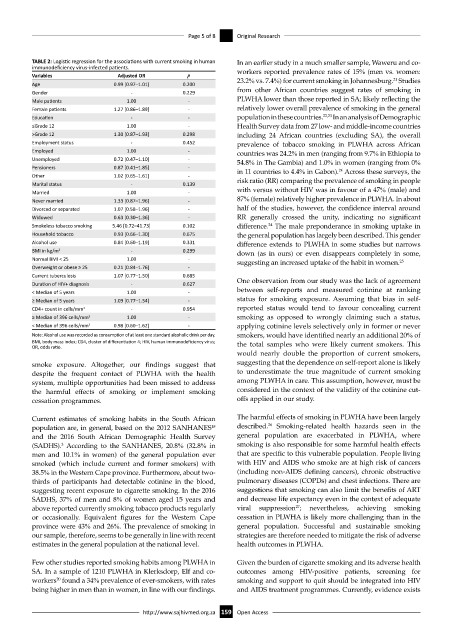
TABLE 2: Logistic regression for the associations with current smoking in human In an earlier study in a much smaller sample, Waweru and co-
immunodeficiency virus-infected patients. workers reported prevalence rates of 15% (men vs. women:
Variables Adjusted OR p 21
Age 0.99 [0.97–1.01] 0.200 23.2% vs. 7.4%) for current smoking in Johannesburg. Studies
Gender - 0.229 from other African countries suggest rates of smoking in
Male patients 1.00 - PLWHA lower than those reported in SA; likely reflecting the
Female patients 1.27 [0.86–1.89] - relatively lower overall prevalence of smoking in the general
Education - - population in these countries. 22,23 In an analysis of Demographic
≤Grade 12 1.00 - Health Survey data from 27 low- and middle-income countries
>Grade 12 1.30 [0.87–1.93] 0.298 including 24 African countries (excluding SA), the overall
Employment status - 0.452 prevalence of tobacco smoking in PLWHA across African
Employed 1.00 - countries was 24.2% in men (ranging from 9.7% in Ethiopia to
Unemployed 0.72 [0.47–1.10] - 54.8% in The Gambia) and 1.0% in women (ranging from 0%
Pensioners 0.87 [0.41–1.85] - in 11 countries to 4.4% in Gabon). Across these surveys, the
24
Other 1.02 [0.65–1.61] -
Marital status - 0.139 risk ratio (RR) comparing the prevalence of smoking in people
Married 1.00 - with versus without HIV was in favour of a 47% (male) and
Never married 1.33 [0.87–1.96] - 87% (female) relatively higher prevalence in PLWHA. In about
Divorced or separated 1.07 [0.58–1.96] - half of the studies, however, the confidence interval around
Widowed 0.63 [0.30–1.36] - RR generally crossed the unity, indicating no significant
24
Smokeless tobacco smoking 5.46 [0.72–41.73] 0.102 difference. The male preponderance in smoking uptake in
Household tobacco 0.93 [0.66–1.30] 0.675 the general population has largely been described. This gender
Alcohol use 0.84 [0.60–1.19] 0.331 difference extends to PLWHA in some studies but narrows
BMI in kg/m 2 - 0.299 down (as in ours) or even disappears completely in some,
Normal BMI ˂ 25 1.00 - suggesting an increased uptake of the habit in women. 25
Overweight or obese ≥ 25 0.21 [0.84–1.76] -
Current tuberculosis 1.07 [0.77–1.50] 0.685
Duration of HIV+ diagnosis - 0.627 One observation from our study was the lack of agreement
< Median of 5 years 1.00 - between self-reports and measured cotinine at ranking
≥ Median of 5 years 1.09 [0.77–1.54] - status for smoking exposure. Assuming that bias in self-
CD4+ count in cells/mm 3 - 0.954 reported status would tend to favour concealing current
≥ Median of 396 cells/mm 3 1.00 - smoking as opposed to wrongly claiming such a status,
< Median of 396 cells/mm 3 0.98 [0.60–1.62] - applying cotinine levels selectively only in former or never
Note: Alcohol use was recorded as consumption of at least one standard alcoholic drink per day. smokers, would have identified nearly an additional 20% of
BMI, body mass index; CD4, cluster of differentiation 4; HIV, human immunodeficiency virus; the total samples who were likely current smokers. This
OR, odds ratio.
would nearly double the proportion of current smokers,
smoke exposure. Altogether, our findings suggest that suggesting that the dependence on self-report alone is likely
despite the frequent contact of PLWHA with the health to underestimate the true magnitude of current smoking
system, multiple opportunities had been missed to address among PLWHA in care. This assumption, however, must be
the harmful effects of smoking or implement smoking considered in the context of the validity of the cotinine cut-
cessation programmes. offs applied in our study.
Current estimates of smoking habits in the South African The harmful effects of smoking in PLWHA have been largely
26
population are, in general, based on the 2012 SANHANES described. Smoking-related health hazards seen in the
18
and the 2016 South African Demographic Health Survey general population are exacerbated in PLWHA, where
(SADHS). According to the SANHANES, 20.8% (32.8% in smoking is also responsible for some harmful health effects
3
men and 10.1% in women) of the general population ever that are specific to this vulnerable population. People living
smoked (which include current and former smokers) with with HIV and AIDS who smoke are at high risk of cancers
38.5% in the Western Cape province. Furthermore, about two- (including non-AIDS defining cancers), chronic obstructive
thirds of participants had detectable cotinine in the blood, pulmonary diseases (COPDs) and chest infections. There are
suggesting recent exposure to cigarette smoking. In the 2016 suggestions that smoking can also limit the benefits of ART
SADHS, 37% of men and 8% of women aged 15 years and and decrease life expectancy even in the context of adequate
27
above reported currently smoking tobacco products regularly viral suppression ; nevertheless, achieving smoking
or occasionally. Equivalent figures for the Western Cape cessation in PLWHA is likely more challenging than in the
province were 43% and 26%. The prevalence of smoking in general population. Successful and sustainable smoking
our sample, therefore, seems to be generally in line with recent strategies are therefore needed to mitigate the risk of adverse
estimates in the general population at the national level. health outcomes in PLWHA.
Few other studies reported smoking habits among PLWHA in Given the burden of cigarette smoking and its adverse health
SA. In a sample of 1210 PLWHA in Klerksdorp, Elf and co- outcomes among HIV-positive patients, screening for
20
workers found a 34% prevalence of ever-smokers, with rates smoking and support to quit should be integrated into HIV
being higher in men than in women, in line with our findings. and AIDS treatment programmes. Currently, evidence exists
http://www.sajhivmed.org.za 159 Open Access