
Page 123 - HIVMED_v21_i1.indb
P. 123
Page 32 of 34 Guideline
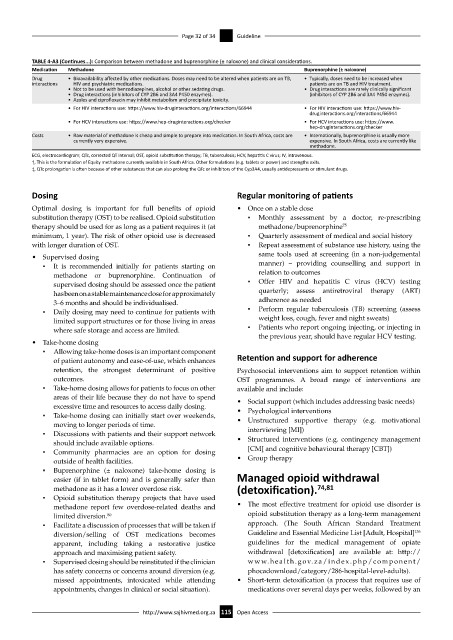
TABLE 4-A3 (Continues...): Comparison between methadone and buprenorphine (± naloxone) and clinical considerations.
Medication Methadone Buprenorphine (± naloxone)
Drug • Bioavailability affected by other medications. Doses may need to be altered when patients are on TB, • Typically, doses need to be increased when
interactions HIV and psychiatric medications. patients are on TB and HIV treatment.
• Not to be used with benzodiazepines, alcohol or other sedating drugs. • Drug interactions are rarely clinically significant
• Drug interactions (inhibitors of CYP 2B6 and 3A4 P450 enzymes). (inhibitors of CYP 2B6 and 3A4 P450 enzymes).
• Azoles and ciprofloxacin may inhibit metabolism and precipitate toxicity.
• For HIV interactions use: https://www.hiv-druginteractions.org/interactions/66944 • For HIV interactions use: https://www.hiv-
druginteractions.org/interactions/66944
• For HCV interactions use: https://www.hep-druginteractions.org/checker • For HCV interactions use: https://www.
hep-druginteractions.org/checker
Costs • Raw material of methadone is cheap and simple to prepare into medication. In South Africa, costs are • Internationally, buprenorphine is usually more
currently very expensive. expensive. In South Africa, costs are currently like
methadone.
ECG, electrocardiogram; QTc, corrected QT interval; OST, opioid substitution therapy; TB, tuberculosis; HCV, hepatitis C virus; IV, intravenous.
†, This is the formulation of Equity methadone currently available in South Africa. Other formulations (e.g. tablets or power) and strengths exits.
‡, QTc prolongation is often because of other substances that can also prolong the QTc or inhibitors of the Cyp3A4, usually antidepressants or stimulant drugs.
Dosing Regular monitoring of patients
Optimal dosing is important for full benefits of opioid • Once on a stable dose
substitution therapy (OST) to be realised. Opioid substitution ▪ Monthly assessment by a doctor, re-prescribing
therapy should be used for as long as a patient requires it (at methadone/buprenorphine 75
minimum, 1 year). The risk of other opioid use is decreased ▪ Quarterly assessment of medical and social history
with longer duration of OST. ▪ Repeat assessment of substance use history, using the
• Supervised dosing same tools used at screening (in a non-judgemental
▪ It is recommended initially for patients starting on manner) – providing counselling and support in
methadone or buprenorphine. Continuation of relation to outcomes
supervised dosing should be assessed once the patient ▪ Offer HIV and hepatitis C virus (HCV) testing
has been on a stable maintenance dose for approximately quarterly; assess antiretroviral therapy (ART)
3–6 months and should be individualised. adherence as needed
▪ Daily dosing may need to continue for patients with ▪ Perform regular tuberculosis (TB) screening (assess
limited support structures or for those living in areas weight loss, cough, fever and night sweats)
where safe storage and access are limited. ▪ Patients who report ongoing injecting, or injecting in
the previous year, should have regular HCV testing.
• Take-home dosing
▪ Allowing take-home doses is an important component
of patient autonomy and ease-of-use, which enhances Retention and support for adherence
retention, the strongest determinant of positive Psychosocial interventions aim to support retention within
outcomes. OST programmes. A broad range of interventions are
▪ Take-home dosing allows for patients to focus on other available and include:
areas of their life because they do not have to spend • Social support (which includes addressing basic needs)
excessive time and resources to access daily dosing.
▪ Take-home dosing can initially start over weekends, • Psychological interventions
• Unstructured supportive therapy (e.g. motivational
moving to longer periods of time.
▪ Discussions with patients and their support network interviewing [MI])
should include available options. • Structured interventions (e.g. contingency management
▪ Community pharmacies are an option for dosing [CM] and cognitive behavioural therapy [CBT])
outside of health facilities. • Group therapy
▪ Buprenorphine (± naloxone) take-home dosing is
easier (if in tablet form) and is generally safer than Managed opioid withdrawal
methadone as it has a lower overdose risk. (detoxification). 74,81
▪ Opioid substitution therapy projects that have used
methadone report few overdose-related deaths and • The most effective treatment for opioid use disorder is
limited diversion. opioid substitution therapy as a long-term management
80
▪ Facilitate a discussion of processes that will be taken if approach. (The South African Standard Treatment
136
diversion/selling of OST medications becomes Guideline and Essential Medicine List [Adult, Hospital]
apparent, including taking a restorative justice guidelines for the medical management of opiate
approach and maximising patient safety. withdrawal [detoxification] are available at: http://
▪ Supervised dosing should be reinstituted if the clinician www.health.gov.za/index.php/component/
has safety concerns or concerns around diversion (e.g. phocadownload/category/286-hospital-level-adults).
missed appointments, intoxicated while attending • Short-term detoxification (a process that requires use of
appointments, changes in clinical or social situation). medications over several days per weeks, followed by an
http://www.sajhivmed.org.za 115 Open Access