
Page 36 - SAHCS HIVMed Journal Vol 20 No 1 2019
P. 36
Page 7 of 26 Guideline
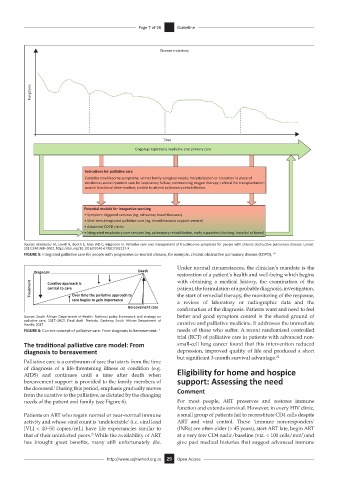
Disease trajectory
Fung
ons
Time
Ongoing respiratory medicine and primary care
Indica ons for pallia ve care
Complex troublesome symptoms; unmet family caregiver needs; hospitalisa
on or transi
on in place of
residence; acute inpa
ent care for respiratory failure; commencing oxygen therapy; referral for transplanta
on;
accute func
onal deteriora
on; unable to a end pulmonary rehabilita
on
Poten al models for integra ve working
• Symptom triggered services (eg, refractory breathlessness)
• Shot-term integrated pallia
ve care (eg, breathlessness support service)
• Advanced COPD clinics
• Integrated respiratory care services (eg, pulmonary rehabilita
on, early supported discharg, hospital at home)
Source: Maddocks M, Lovell N, Booth S, Man WD-C, Higginson IJ. Palliative care and management of troublesome symptoms for people with chronic obstructive pulmonary disease. Lancet.
2017;390:988–1002. https://doi.org/10.1016/S0140-6736(17)32127-X
FIGURE 5: Integrated palliative care for people with progressive co-morbid disease, for example, chronic obstructive pulmonary disease (COPD). 19
Under normal circumstances, the clinician’s mandate is the
Diagnosis Death
restoration of a patient’s health and well-being which begins
with obtaining a medical history, the examination of the
Treatment Cura ve approach is patient, the formulation of a probable diagnosis, investigation,
central to care
the start of remedial therapy, the monitoring of the response,
Over me the pallia ve approach to
care begins to gain importance
a review of laboratory or radiographic data and the
Bereavement care confirmation of the diagnosis. Patients want and need to feel
Source: South African Department of Health. National policy framework and strategy on better and good symptom control is the shared ground of
palliative care, 2017–2022. Final draft. Pretoria, Gauteng: South African Department of
Health; 2017 curative and palliative medicine. It addresses the immediate
FIGURE 6: Current concept of palliative care: From diagnosis to bereavement. 1 needs of those who suffer. A recent randomised controlled
trial (RCT) of palliative care in patients with advanced non-
The traditional palliative care model: From small-cell lung cancer found that this intervention reduced
diagnosis to bereavement depression, improved quality of life and produced a short
but significant 3-month survival advantage. 22
Palliative care is a continuum of care that starts from the time
of diagnosis of a life-threatening illness or condition (e.g. Eligibility for home and hospice
AIDS) and continues until a time after death when
bereavement support is provided to the family members of support: Assessing the need
the deceased. During this period, emphasis gradually moves Comment
1
from the curative to the palliative, as dictated by the changing
needs of the patient and family (see Figure 6). For most people, ART preserves and restores immune
function and extends survival. However, in every HIV clinic,
Patients on ART who regain normal or near-normal immune a small group of patients fail to reconstitute CD4 cells despite
activity and whose viral count is ‘undetectable’ (i.e. viral load ART and viral control. These ‘immune non-responders’
[VL] < 40–50 copies/mL) have life expectancies similar to (INRs) are often older (> 45 years), start ART late, begin ART
that of their uninfected peers. While the availability of ART at a very low CD4 nadir/baseline (viz. < 100 cells/mm ) and
21
3
has brought great benefits, many still unfortunately die. give past medical histories that suggest advanced immune
http://www.sajhivmed.org.za 29 Open Access