
Page 31 - SAHCS HIVMed Journal Vol 20 No 1 2019
P. 31
Page 2 of 26 Guideline
Do HIV-infected South Africans need the routine background of care. From time to time, this
palliative care? Figure 1 routine is interrupted by disease. This necessitates a shift
in the emphasis of care. Palliation becomes an option for
Human immunodeficiency virus infection is incurable. those with incurable conditions, such as a central nervous
About 770 000 people died of HIV worldwide in 2018. More system (CNS) lymphoma, disabling stroke, renal and liver
than two-thirds of these died in Africa (UNAIDS Global Aids failure, et cetera. For PLWHIV who live longer, the
Update 2019). Although Statistics South Africa has recorded diseases of old age, for example, chronic lung conditions,
some improvement in the overall survival, HIV-related levels diabetes, cardiovascular disease, bone fragility,
of morbidity and mortality remain high. Mortality is greatest neurocognitive decline, and the non-AIDS defining
among those not on antiretroviral therapy (ART), that is, cancers, emerge. Indeed, these conditions generally
either naïve to ART or those who have stopped taking appear a decade or more before identical disease affects
medication and are outside of care. Mortality is also high in uninfected peers (see Figures 4, 5 and 6).
the first year after the start of ART. Of South Africa’s 7.97
million people living with HIV (PLWHIV) in 2019, only 4.94 Formal assessment of the need for
million are on ART. A detectable viral load while on ART is palliative care
usually a sign of treatment failure or poor viral control. These
persons are also at increased risk of HIV-related morbidity Limited resources in the face of huge demand necessitate an
and mortality. equitable system of patient triage. With regard to the private
funding of costly care options, such as hospice admission
Models of palliative care and home nursing, these guidelines recommend the
SPICT Tm Tool (Appendix 2) and the VACS SCORE criteria
• No palliative care: Access to formal palliative care within (Appendix 3) to be followed as a guide to eligibility. These
either the public or private health sector in much of Africa assessment tools are accredited internationally and with
including SA, is extremely limited. Few currently access minor adaptation can be used in the South African context.
this care (see Figure 3 and Appendix 1).
• The traditional model of palliative care: In this scenario,
curative care and palliative care are available to the patient The symptomatic management of
at the time of diagnosis. Curative care is initially given HIV-infected people receiving
priority. But when curative options are exhausted, palliative care
palliation offers an alternative approach, one that grows in
importance as time passes. Despite four decades of HIV The core activity of the palliative care team and its clinician(s)
research, a cure remains out of reach. In these circumstances, is the relief of suffering. Pain, particularly chronic pain
health facilities and healthcare workers must be trained to lasting ≥ 3 months, is experienced by the majority of
provide palliative care to those in need of it. PLWHIV before death. A formal approach to the assessment
• The long-term model of HIV palliative care: In this scenario, of both acute and chronic pain underlies its successful
ART, prophylactic trimethoprim-sulfamethoxazole, management (see Table 2). Pain control is not always
isoniazid (INH) and vaccination against influenza, the achieved. However, it is more likely if theoretic knowledge
pneumococcus, hepatitis B and regular clinic visits form is supplemented with bedside experience. In this regard, the
2017 Guideline on the Management of Chronic Pain from the
HIV Division of the Infectious Diseases Society of America
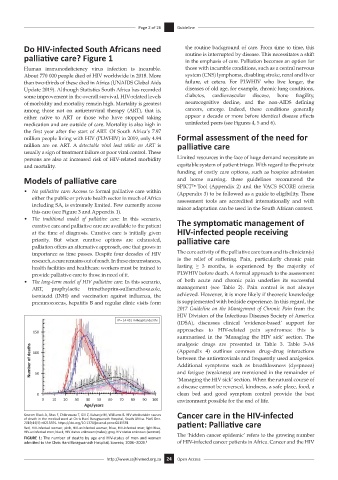
N = 14 431 in-hospital deaths
(IDSA), discusses clinical ‘evidence-based’ support for
approaches to HIV-related pain syndromes: this is
150
summarised in the ‘Managing the HIV sick’ section. The
analgesic drugs are presented in Table 3. Table 3-A6
Number of deaths 100 (Appendix 4) outlines common drug–drug interactions
between the antiretrovirals and frequently used analgesics.
Additional symptoms such as breathlessness (dyspnoea)
and fatigue (weakness) are mentioned in the remainder of
50
‘Managing the HIV sick’ section. When the natural course of
a disease cannot be reversed, kindness, a safe place, food, a
0 clean bed and good symptom control provide the best
0 10 20 30 40 50 60 70 80 90 100 environment possible for the end of life.
Age/years
Source: Black A, Sitas F, Chibrawara T, Gill Z, Kubanje M, Williams B. HIV-attributable causes Cancer care in the HIV-infected
of death in the medical ward at Chris Hani Baragwanath Hospital, South Africa. PLoS One.
2019;14(5):e0215591. https://doi.org/10.1371/journal.pone.0215591 patient: Palliative care
Red, HIV-infected women; pink, HIV-uninfected women; blue, HIV-infected men; light blue,
HIV-uninfected men; black, HIV status unknown (males); grey, HIV status unknown (women). The ‘hidden cancer epidemic’ refers to the growing number
FIGURE 1: The number of deaths by age and HIV-status of men and women
admitted to the Chris Hani Baragwanath Hospital, Soweto, 2006–2009. 8 of HIV-infected cancer patients in Africa. Cancer and the HIV
http://www.sajhivmed.org.za 24 Open Access