
Page 294 - HIVMED_v21_i1.indb
P. 294
Page 4 of 10 Original Research
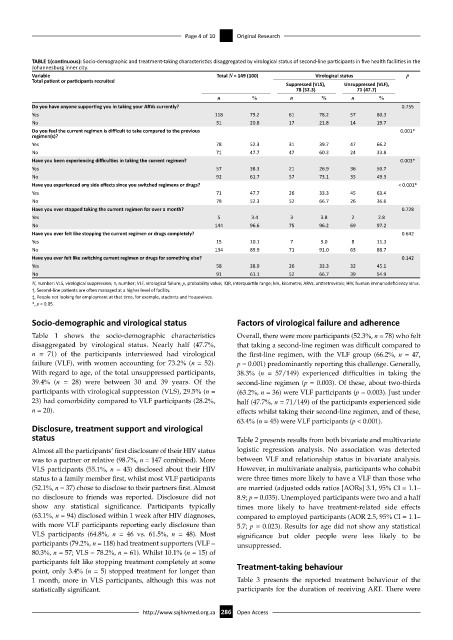
TABLE 1(continuous): Socio-demographic and treatment-taking characteristics disaggregated by virological status of second-line participants in five health facilities in the
Johannesburg inner city.
Variable Total N = 149 (100) Virological status p
Total patient or participants recruited
Suppressed (VLS), Unsuppressed (VLF),
78 (52.3) 71 (47.7)
n % n % n %
Do you have anyone supporting you in taking your ARVs currently? 0.755
Yes 118 79.2 61 78.2 57 80.3
No 31 20.8 17 21.8 14 19.7
Do you feel the current regimen is difficult to take compared to the previous 0.001*
regimen(s)?
Yes 78 52.3 31 39.7 47 66.2
No 71 47.7 47 60.3 24 33.8
Have you been experiencing difficulties in taking the current regimen? 0.003*
Yes 57 38.3 21 26.9 36 50.7
No 92 61.7 57 73.1 35 49.3
Have you experienced any side effects since you switched regimens or drugs? < 0.001*
Yes 71 47.7 26 33.3 45 63.4
No 78 52.3 52 66.7 26 36.6
Have you ever stopped taking the current regimen for over a month? 0.728
Yes 5 3.4 3 3.8 2 2.8
No 144 96.6 75 96.2 69 97.2
Have you ever felt like stopping the current regimen or drugs completely? 0.642
Yes 15 10.1 7 9.0 8 11.3
No 134 89.9 71 91.0 63 88.7
Have you ever felt like switching current regimen or drugs for something else? 0.142
Yes 58 38.9 26 33.3 32 45.1
No 91 61.1 52 66.7 39 54.9
N, number; VLS, virological suppression; n, number; VLF, virological failure; p, probability value; IQR, interquartile range; km, kilometre; ARVs, antiretrovirals; HIV, human immunodeficiency virus.
†, Second-line patients are often managed at a higher level of facility.
‡, People not looking for employment at that time, for example, students and housewives.
*, p < 0.05.
Socio-demographic and virological status Factors of virological failure and adherence
Table 1 shows the socio-demographic characteristics Overall, there were more participants (52.3%, n = 78) who felt
disaggregated by virological status. Nearly half (47.7%, that taking a second-line regimen was difficult compared to
n = 71) of the participants interviewed had virological the first-line regimen, with the VLF group (66.2%, n = 47,
failure (VLF), with women accounting for 73.2% (n = 52). p = 0.001) predominantly reporting this challenge. Generally,
With regard to age, of the total unsuppressed participants, 38.3% (n = 57/149) experienced difficulties in taking the
39.4% (n = 28) were between 30 and 39 years. Of the second-line regimen (p = 0.003). Of these, about two-thirds
participants with virological suppression (VLS), 29.5% (n = (63.2%, n = 36) were VLF participants (p = 0.003). Just under
23) had comorbidity compared to VLF participants (28.2%, half (47.7%, n = 71/149) of the participants experienced side
n = 20). effects whilst taking their second-line regimen, and of these,
63.4% (n = 45) were VLF participants (p < 0.001).
Disclosure, treatment support and virological
status Table 2 presents results from both bivariate and multivariate
Almost all the participants’ first disclosure of their HIV status logistic regression analysis. No association was detected
was to a partner or relative (98.7%, n = 147 combined). More between VLF and relationship status in bivariate analysis.
VLS participants (55.1%, n = 43) disclosed about their HIV However, in multivariate analysis, participants who cohabit
status to a family member first, whilst most VLF participants were three times more likely to have a VLF than those who
(52.1%, n = 37) chose to disclose to their partners first. Almost are married (adjusted odds ratios [AORs] 3.1, 95% CI = 1.1–
no disclosure to friends was reported. Disclosure did not 8.9; p = 0.035). Unemployed participants were two and a half
show any statistical significance. Participants typically times more likely to have treatment-related side effects
(63.1%, n = 94) disclosed within 1 week after HIV diagnoses, compared to employed participants (AOR 2.5, 95% CI = 1.1–
with more VLF participants reporting early disclosure than 5.7; p = 0.023). Results for age did not show any statistical
VLS participants (64.8%, n = 46 vs. 61.5%, n = 48). Most significance but older people were less likely to be
participants (79.2%, n = 118) had treatment supporters (VLF = unsuppressed.
80.3%, n = 57; VLS = 78.2%, n = 61). Whilst 10.1% (n = 15) of
participants felt like stopping treatment completely at some Treatment-taking behaviour
point, only 3.4% (n = 5) stopped treatment for longer than
1 month, more in VLS participants, although this was not Table 3 presents the reported treatment behaviour of the
statistically significant. participants for the duration of receiving ART. There were
http://www.sajhivmed.org.za 286 Open Access