
Page 243 - HIVMED_v21_i1.indb
P. 243
Page 5 of 9 Review Article
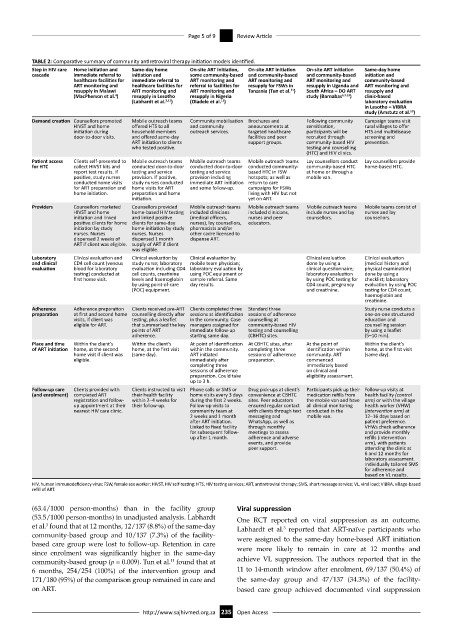
TABLE 2: Comparative summary of community antiretroviral therapy initiation models identified.
Step in HIV care Home initiation and Same-day home On-site ART initiation, On-site ART initiation On-site ART initiation Same-day home
cascade immediate referral to initiation and some community-based and community-based and community-based initiation and
healthcare facilities for immediate referral to ART monitoring and ART monitoring and ART monitoring and community-based
ART monitoring and healthcare facilities for referral to facilities for resupply for FSWs in resupply in Uganda and ART monitoring and
11
resupply in Malawi ART monitoring and ART monitoring and Tanzania (Tun et al. ) South Africa – DO ART resupply and
(MacPherson et al. ) 4 resupply in Lesotho resupply in Nigeria study (Barnabas 6,7,13 ) clinic-based
(Labhardt et al. 3,12 ) (Oladele et al. ) laboratory evaluation
11
in Lesotho – VIBRA
10
study (Amstutz et al. )
Demand creation Counsellors promoted Mobile outreach teams Community mobilisation Brochures and Following community Campaign teams visit
HIVST and home offered HTS to all and community announcements at sensitisation, rural villages to offer
initiation during household members outreach services. targeted healthcare participants will be HTS and multidisease
door-to-door visits. and offered same-day facilities and peer recruited through screening and
ART initiation to clients support groups. community-based HIV prevention.
who tested positive. testing and counselling
(HTC) and HIV clinics.
Patient access Clients self-presented to Mobile outreach teams Mobile outreach teams Mobile outreach teams Lay counsellors conduct Lay counsellors provide
for HTC collect HIVST kits and conducted door-to-door conducted door-to-door conducted community- community-based HTC home-based HTC.
report test results. If testing and service testing and service based HTC in FSW at home or through a
positive, study nurses provision. If positive, provision including hotspots; as well as mobile van.
conducted home visits study nurses conducted immediate ART initiation return to care
for ART preparation and home visits for ART and some follow-up. campaigns for FSWs
home initiation. preparation and home living with HIV but not
initiation. yet on ART.
Providers Counsellors marketed Counsellors provided Mobile outreach teams Mobile outreach teams Mobile outreach teams Mobile teams consist of
HIVST and home home-based HIV testing included clinicians included clinicians, include nurses and lay nurses and lay
initiation and linked and linked positive (medical officers, nurses and peer counsellors. counsellors.
positive clients for home clients for same-day nurses), lay counsellors, educators.
initiation by study home initiation by study pharmacists and/or
nurses. Nurses nurses. Nurses other cadre licensed to
dispensed 2 weeks of dispensed 1 month dispense ART.
ART if client was eligible. supply of ART if client
was eligible.
Laboratory Clinical evaluation and Clinical evaluation by Clinical evaluation by Clinical evaluation Clinical evaluation
and clinical CD4 cell count (venous study nurse; laboratory mobile team physician; done by using a (medical history and
evaluation blood for laboratory evaluation including CD4 laboratory evaluation by clinical questionnaire; physical examination)
testing) conducted at cell counts, creatinine using POC equipment or laboratory evaluation done by using a
first home visit. levels and haemoglobin sample referral. Same by using POC testing for checklist; laboratory
by using point-of-care day results. CD4 count, pregnancy evaluation by using POC
(POC) equipment. and creatinine. testing for CD4 count,
haemoglobin and
creatinine.
Adherence Adherence preparation Clients received pre-ART Clients completed three Standard three Study nurse conducts a
preparation at first and second home counselling directly after sessions at identification sessions of adherence one-on-one structured
visits, if client was testing, plus a leaflet in the community. Case counselling at education and
eligible for ART. that summarised the key managers assigned for community-based HIV counselling session
points of ART immediate follow-up testing and counselling by using a leaflet
adherence. starting same day. (CBHTC) sites. (5–10 min).
Place and time Within the client’s Within the client’s At point of identification At CBHTC sites, after At the point of Within the client’s
of ART initiation home, at the second home, at the first visit within the community. completing three identification within home, at the first visit
home visit if client was (same day). ART initiated sessions of adherence community. ART (same day).
eligible. immediately after preparation. commenced
completing three immediately based
sessions of adherence on clinical and
preparation. Could take eligibility assessment.
up to 3 h.
Follow-up care Clients provided with Clients instructed to visit Phone calls or SMS or Drug pick-ups at client’s Participants pick up their Follow-up visits at
(and enrolment) completed ART their health facility home visits every 3 days convenience at CBHTC medication refills from health facility (control
registration and follow- within 2–4 weeks for during the first 2 weeks. sites. Peer educators the mobile van and have arm) or with the village
up appointment at their their follow-up. Follow-up visits to ensured regular contact all clinical monitoring health worker (VHW)
nearest HIV care clinic. community team at with clients through text conducted in the (intervention arm) at
2 weeks and 1 month messaging and mobile van. 12–16 days based on
after ART initiation. WhatsApp, as well as patient preference.
Linked to fixed facility through monthly VHWs check adherence
for subsequent follow- meetings to assess and provide monthly
up after 1 month. adherence and adverse refills (intervention
events, and provide arm), with patients
peer support. attending the clinic at
6 and 12 months for
laboratory assessment.
Individually tailored SMS
for adherence and
based on VL results.
HIV, human immunodeficiency virus; FSW, female sex worker; HIVST, HIV self-testing; HTS, HIV testing services; ART, antiretroviral therapy; SMS, short message service; VL, viral load; VIBRA, village-based
refill of ART.
(63.4/1000 person-months) than in the facility group Viral suppression
(53.5/1000 person-months) in unadjusted analysis. Labhardt One RCT reported on viral suppression as an outcome.
et al. found that at 12 months, 12/137 (8.8%) of the same-day Labhardt et al. reported that ART-naïve participants who
3
3
community-based group and 10/137 (7.3%) of the facility- were assigned to the same-day home-based ART initiation
based care group were lost to follow-up. Retention in care were more likely to remain in care at 12 months and
since enrolment was significantly higher in the same-day
community-based group (p = 0.009). Tun et al. found that at achieve VL suppression. The authors reported that in the
11
6 months, 254/254 (100%) of the intervention group and 11 to 14-month window after enrolment, 69/137 (50.4%) of
171/180 (95%) of the comparison group remained in care and the same-day group and 47/137 (34.3%) of the facility-
on ART. based care group achieved documented viral suppression
http://www.sajhivmed.org.za 235 Open Access