
Page 241 - HIVMED_v21_i1.indb
P. 241
Page 3 of 9 Review Article
patient population and outcome measures. The secondary Tanzania and Uganda. The four completed studies were
reviewer reviewed all the extractions for accuracy. assessed by using the McMaster University’s Quality
Assessment Tool, and individual studies ranged in quality
Quality evidence assessment and from 1 (strong) to 3 (weak), with the overall average being 2.
risk of bias The two ongoing RCTs included in the model description
were not assessed for quality as they had not been completed
The quality of evidence and risk of bias (RoB) of the studies at the time of reporting.
included in the final review was assessed by one reviewer by
using the McMaster University’s Quality Assessment Tool Models of community-based antiretroviral
(https://merst.ca/ephpp-tools/) from the Effective Public therapy initiation
Health Practice Project (EPHPP). The secondary reviewer Community-based ART initiation modalities include home,
verified the quality of evidence and the RoB assessment.
mobile and workplace as part of an HIV-testing campaign.
The review identified two main models of CB-ARTi, with
Ethical consideration some variations across countries (Table 2): (1) on-site ART
This article followed all ethical standards for research without initiation and community-based ART monitoring and
direct contact with human or animal subjects. resupply 7,9,10 and (2) a hybrid model with on-site community
ART initiation and referral to local clinics for ART monitoring
Results and resupply. 3,4,11 In addition, the review identified key
Study selection and characteristics of activities addressing seven areas of CB-ARTi service delivery,
namely (1) demand creation, (2) patient access for HTC, (3)
included studies provider roles, including task shifting, (4) laboratory and
The process of study identification and selection concluded clinical evaluation, (5) adherence preparation, (6) place and
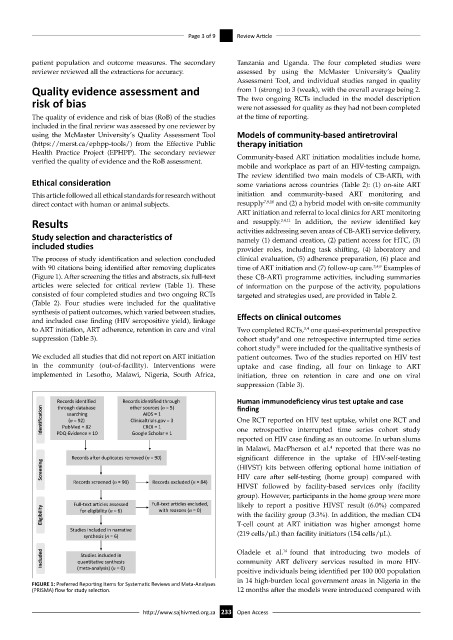
with 90 citations being identified after removing duplicates time of ART initiation and (7) follow-up care. 3,4,9 Examples of
(Figure 1). After screening the titles and abstracts, six full-text these CB-ARTi programme activities, including summaries
articles were selected for critical review (Table 1). These of information on the purpose of the activity, populations
consisted of four completed studies and two ongoing RCTs targeted and strategies used, are provided in Table 2.
(Table 2). Four studies were included for the qualitative
synthesis of patient outcomes, which varied between studies, Effects on clinical outcomes
and included case finding (HIV seropositive yield), linkage
to ART initiation, ART adherence, retention in care and viral Two completed RCTs, one quasi-experimental prospective
3,4
suppression (Table 3). cohort study and one retrospective interrupted time series
9
11
cohort study were included for the qualitative synthesis of
We excluded all studies that did not report on ART initiation patient outcomes. Two of the studies reported on HIV test
in the community (out-of-facility). Interventions were uptake and case finding, all four on linkage to ART
implemented in Lesotho, Malawi, Nigeria, South Africa, initiation, three on retention in care and one on viral
suppression (Table 3).
Records identified Records identified through Human immunodeficiency virus test uptake and case
other sources (n = 5)
finding
through database
Identification PubMed = 82 Clinicaltrials.gov = 3 One RCT reported on HIV test uptake, whilst one RCT and
AIDS = 1
searching
(n = 92)
CROI = 1
one retrospective interrupted time series cohort study
Google Scholar = 1
PDQ-Evidence = 10
reported on HIV case finding as an outcome. In urban slums
in Malawi, MacPherson et al. reported that there was no
4
Records after duplicates removed (n = 90) significant difference in the uptake of HIV-self-testing
Screening (HIVST) kits between offering optional home initiation of
Records screened (n = 90) Records excluded (n = 84) HIV care after self-testing (home group) compared with
HIVST followed by facility-based services only (facility
group). However, participants in the home group were more
Full-text articles assessed Full-text articles excluded, likely to report a positive HIVST result (6.0%) compared
Eligibility for eligibility (n = 6) with reasons (n = 0) with the facility group (3.3%). In addition, the median CD4
Studies included in narrative T-cell count at ART initiation was higher amongst home
(219 cells/µL) than facility initiators (154 cells/µL).
synthesis (n = 6)
Included quantitative synthesis Oladele et al. 14 found that introducing two models of
Studies included in
community ART delivery services resulted in more HIV-
(meta-analysis) (n = 0)
positive individuals being identified per 100 000 population
in 14 high-burden local government areas in Nigeria in the
FIGURE 1: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
(PRISMA) flow for study selection. 12 months after the models were introduced compared with
http://www.sajhivmed.org.za 233 Open Access