
Page 173 - HIVMED_v21_i1.indb
P. 173
Page 3 of 6 Original Research
relationships, reduce avoidant responses to distressing TABLE 1: Demographic characteristics.
experiences and facilitate successful implementation of Characteristic N or Median % or IQR
smoking trigger management strategies. Sessions 3–5 Age in years 39.5 34, 48
incorporate strategies to address avoidance patterns, Male candidates 38 95
especially those involving smoking, and replace them with Number of cigarettes per day 10 6, 11.5
-
-
FTND category at enrolment (week 0)
adaptive coping strategies, again by using problem solving. Low dependence (1–2) 0 -
Sessions were conducted by telephone over a 12-week period Low-to-moderate dependence (3–4) 0 -
(with the first session lasting 1 h and subsequent sessions Moderate dependence (5–7) 37 92.5
lasting 30–45 min on average) and involved weekly High dependence (≥ 8) 3 7.5
homework assignments. SHAPS score at enrolment 1.5 0.5, 2.5
SHAPS score > 2 10 25
Data collection and management IQR, interquartile range; FTND, Fagerstr öm Test for Nicotine Dependence; SHAPS, Snaith–
Hamilton Pleasure Scale (normal = 2 or less; abnormal = 3 or more).
Collected data included information related to smoking
behaviour (including nicotine dependence measured by the
19
Fagerström Test for Nicotine Dependence ), anhedonia Screened for eligibility (n = 128)
[using the Snaith–Hamilton Pleasure Scale (SHAPS) ] and
20
feasibility (e.g., rate of accrual and retention and appeal of
the intervention). Participant accrual rate was defined as the
number of participants enrolled over 8 weeks. Retention was Ineligible (n = 78): < 5 cigs/day
calculated as a proportion of participants enrolled who were
available at week 12 contact session. Study staff not acting as
interventionists interviewed participants at baseline, week 6 Eligible (n = 50)
and week 12 to determine if they were still smoking and
whether they implemented the suggested intervention Declined to par cipate (n = 10)
strategies. The timeline follow-back procedure assessed daily • Not interested (n = 3)
• Privacy issues (n = 3)
smoking between measurement time points. Additionally, • Other reasons (n = 4)
21
the amount of carbon monoxide (CO) in participants’ breath
was tested to confirm self-reported abstinence from tobacco. Enrolled (n = 40)
Data were collected on paper and transferred to an electronic
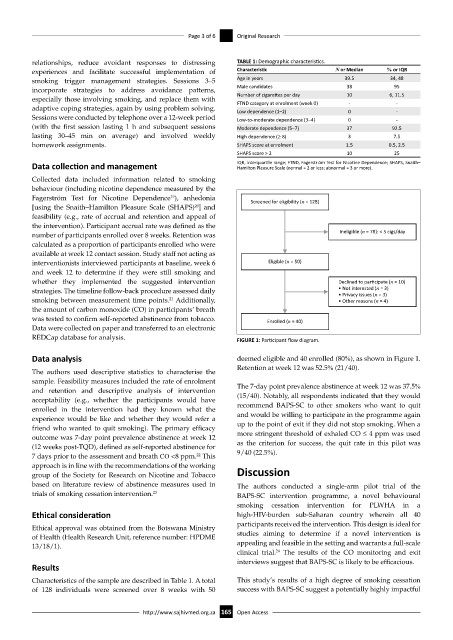
REDCap database for analysis. FIGURE 1: Participant flow diagram.
Data analysis deemed eligible and 40 enrolled (80%), as shown in Figure 1.
Retention at week 12 was 52.5% (21/40).
The authors used descriptive statistics to characterise the
sample. Feasibility measures included the rate of enrolment
and retention and descriptive analysis of intervention The 7-day point prevalence abstinence at week 12 was 37.5%
acceptability (e.g., whether the participants would have (15/40). Notably, all respondents indicated that they would
enrolled in the intervention had they known what the recommend BAPS-SC to other smokers who want to quit
experience would be like and whether they would refer a and would be willing to participate in the programme again
friend who wanted to quit smoking). The primary efficacy up to the point of exit if they did not stop smoking. When a
outcome was 7-day point prevalence abstinence at week 12 more stringent threshold of exhaled CO ≤ 4 ppm was used
(12 weeks post-TQD), defined as self-reported abstinence for as the criterion for success, the quit rate in this pilot was
22
7 days prior to the assessment and breath CO <8 ppm. This 9/40 (22.5%).
approach is in line with the recommendations of the working
group of the Society for Research on Nicotine and Tobacco Discussion
based on literature review of abstinence measures used in The authors conducted a single-arm pilot trial of the
trials of smoking cessation intervention. 23 BAPS-SC intervention programme, a novel behavioural
smoking cessation intervention for PLWHA in a
Ethical consideration high-HIV-burden sub-Saharan country wherein all 40
participants received the intervention. This design is ideal for
Ethical approval was obtained from the Botswana Ministry
of Health (Health Research Unit, reference number: HPDME studies aiming to determine if a novel intervention is
13/18/1). appealing and feasible in the setting and warrants a full-scale
24
clinical trial. The results of the CO monitoring and exit
interviews suggest that BAPS-SC is likely to be efficacious.
Results
Characteristics of the sample are described in Table 1. A total This study’s results of a high degree of smoking cessation
of 128 individuals were screened over 8 weeks with 50 success with BAPS-SC suggest a potentially highly impactful
http://www.sajhivmed.org.za 165 Open Access