
Page 17 - SAHCS HIVMed Journal Vol 20 No 1 2019
P. 17
Page 4 of 16 Guideline
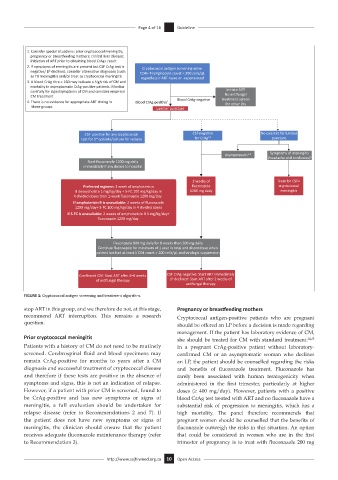
1. Consider special situa ons: prior cryptococcal meningi s;
pregnancy or breaseeding mothers; clinical liver disease;
ini a on of ART prior to obtaining blood CrAg+ result
2. If symptoms of meningi s are present but CSF CrAg test is Cryptococcal an gen screening when
nega ve/ LP declined, consider alterna ve diagnoses (such CD4+ T-lymphocyte count < 200 cells/µL
as TB meningi s) and/or treat as cryptococcal meningi s regardless if ART-naive or -experienced
3. A blood CrAg tre > 160 may indicate a high risk of CM and
mortality in asymptoma c CrAg-posi ve pa ents. Monitor
carefully for signs/symptoms of CM and consider empirical Ini ate ART
No an fungal
CM treatment treatment screen
4. There is no evidence for appropriate ART ming in Blood CrAg-posi ve 1 Blood CrAg-nega ve for other Ols
these groups Lumbar puncture
CSF posi ve for any cryptococcal CSF nega ve No consent for lumbar
test for 1 episode/culture for relapse for CrAg 2,4 puncture
st
Asymptoma c 3,4 Symptoms of meningi s
(headache and confusion) 2
Start fluconazole 1200 mg daily
immediately if any delays to hospital
2 weeks of Treat for CSF+
Preferred regimen: 1 week of amphotericin fluconazole cryptococcal
B deoxycholate 1 mg/kg/day + 5-FC 100 mg/kg/day in 1200 mg daily meningi s
4 divided doses then 1-week fluconazole 1200 mg/day
If amphotericin B is unavailable: 2 weeks of fluconazole
1200 mg/day+ 5-FC 100 mg/kg/day in 4 divided doses
If 5-FC is unavailable: 2 weeks of amphotericin B 1 mg/kg/day+
fluconazole 1200 mg/day
Fluconazole 800 mg daily for 8 weeks then 200 mg daily
Con nue fluconazole for minimum of 1 year in total and discon nue when
pa ent has had at least 1 CD4 count > 200 cells/µL and virologic suppression
Confirmed CM: Start ART aer 4–6 weeks CSF CrAg-nega ve: Start ART immediately
of an fungal therapy LP declined: Start ART aer 2 weeks of
an fungal therapy
FIGURE 1: Cryptococcal antigen screening and treatment algorithm.
stop ART in this group, and we therefore do not, at this stage, Pregnancy or breastfeeding mothers
recommend ART interruption. This remains a research Cryptococcal antigen-positive patients who are pregnant
question.
should be offered an LP before a decision is made regarding
management. If the patient has laboratory evidence of CM,
Prior cryptococcal meningitis she should be treated for CM with standard treatment. 24,25
Patients with a history of CM do not need to be routinely In a pregnant CrAg-positive patient without laboratory-
screened. Cerebrospinal fluid and blood specimens may confirmed CM or an asymptomatic woman who declines
remain CrAg-positive for months to years after a CM an LP, the patient should be counselled regarding the risks
diagnosis and successful treatment of cryptococcal disease and benefits of fluconazole treatment. Fluconazole has
and therefore if these tests are positive in the absence of rarely been associated with human teratogenicity when
symptoms and signs, this is not an indication of relapse. administered in the first trimester, particularly at higher
However, if a patient with prior CM is screened, found to doses (≥ 400 mg/day). However, patients with a positive
be CrAg-positive and has new symptoms or signs of blood CrAg test treated with ART and no fluconazole have a
meningitis, a full evaluation should be undertaken for substantial risk of progression to meningitis, which has a
relapse disease (refer to Recommendations 2 and 7). If high mortality. The panel therefore recommends that
the patient does not have new symptoms or signs of pregnant women should be counselled that the benefits of
meningitis, the clinician should ensure that the patient fluconazole outweigh the risks in this situation. An option
receives adequate fluconazole maintenance therapy (refer that could be considered in women who are in the first
to Recommendation 3). trimester of pregnancy is to treat with fluconazole 200 mg
http://www.sajhivmed.org.za 10 Open Access